Upper airway signs: inspiratory stridor, suprasternal retractions, drooling
e.g., laryngospasm, angioedema , anaphylaxis, tumors, croup , epiglottitis , diphtheria , drowning, OSA
Above the level of the vocal cords: nasal cavity, nasopharynx, oropharynx, hypopharynx, larynx. They are mostly soft tissues, easily to collapse with negative pressure.
Lower airway signs: expiratory wheezing, rhonchi, prolonged exhalation
Stridor
Pathophysiology & Classification
Harsh, high-pitched respiratory sound caused by turbulent airflow through a narrowed upper airway.
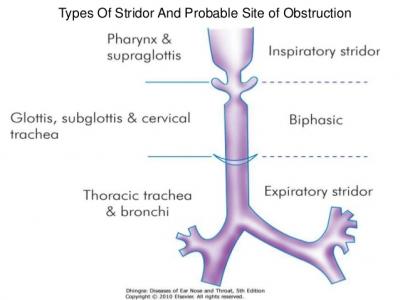
Inspiratory : Extrathoracic obstruction (e.g., larynx, upper trachea).Expiratory : Intrathoracic obstruction (lower trachea).Biphasic : Fixed obstruction (e.g., subglottic stenosis, vascular ring). c
Clinical Features
Red Flags : Drooling, tripod posture, cyanosis, hypoxia, severe retractions, altered mental status (AMS). Indicates impending respiratory failure. Onset: Acute (infectious, allergic, foreign body) vs Chronic (congenital anomalies, tumors).
Diagnosis
Initial : Clinical evaluation (do NOT agitate a pediatric pt with suspected epiglottitis).Imaging : AP/Lateral neck XR (eval for steeple sign, thumbprint sign, radiopaque foreign body).Confirmatory/Gold Standard : Direct laryngoscopy/bronchoscopy (must be done in a controlled setting like the OR if severe obstruction is suspected).
Differential Diagnostics (High-Yield Causes)
Croup (Laryngotracheobronchitis) :
Epi : 6 mo - 3 yrs. Parainfluenza virus.Presentation : Gradual onset, barking cough, hoarseness, coryza.Dx : AP neck XR shows “Steeple sign” (subglottic narrowing).Diff : Non-toxic appearance compared to epiglottitis.
Epiglottitis :
Epi : Unimmunized children (H. influenzae type b) or adults (Strep/Staph ).Presentation : Acute onset, toxic appearance, high fever, drooling, dysphagia, sniffing/tripod position.Dx : Lateral neck XR shows “Thumbprint sign”.Diff : Rapid deterioration, absence of barking cough.
Foreign Body Aspiration (FBA) :
Epi : Toddlers (1-3 yrs).Presentation : Sudden-onset choking, stridor, focal wheezing, asymmetric breath sounds.Dx : Expiratory/decubitus CXR (shows hyperinflation on the affected side due to ball-valve effect).
Bacterial Tracheitis :
Epi : S. aureus following a viral URI/croup.Presentation : Croup-like presentation but pt appears toxic, high fever.Diff : Does not improve with racemic epinephrine (unlike croup).
Laryngomalacia :
Epi : Infants (most common cause of chronic infant stridor).Presentation : Inspiratory stridor that worsens in supine position/during feeding/crying; improves prone.Dx : Direct laryngoscopy (collapse of supraglottic structures during inspiration). Resolves spontaneously by 12-18 mo.
Vascular Ring :
Epi : Congenital (e.g., double aortic arch).Presentation : Biphasic stridor, improves with neck extension. Often presents with dysphagia (“dysphagia lusoria”).
Anaphylaxis :
Epi : Exposure to allergen (food, venom, meds).Presentation : Sudden onset airway edema, wheezing, urticaria, hypotension.