Maternal polyhydramnios (fetus cannot swallow amniotic fluid in utero).
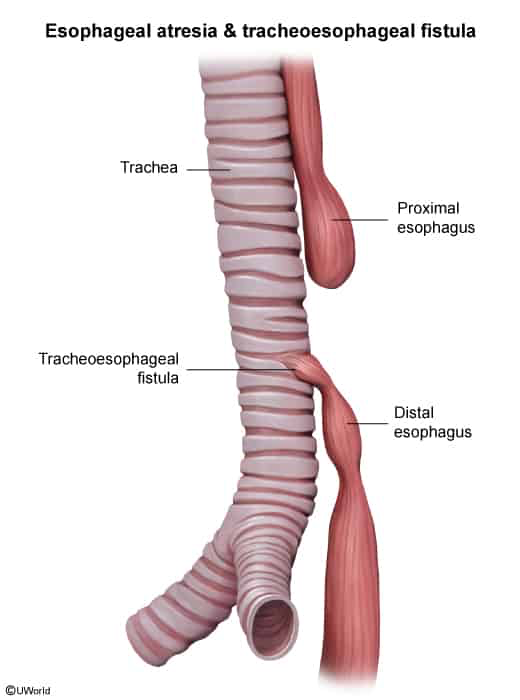
Most common subtype: Type C (esophageal atresia [EA] w/ distal tracheoesophageal fistula [TEF]; ~85% of cases). c
Clinical Features
Excessive drooling and salivation immediately post-delivery. c
Choking, coughing, and cyanosis during the first feeding.
Respiratory distress due to aspiration of saliva or refluxed gastric contents.
Abdominal distension (if distal TEF present, air enters the GI tract during breathing).
Scaphoid abdomen (if pure EA or EA w/ proximal TEF only).
Diagnosis
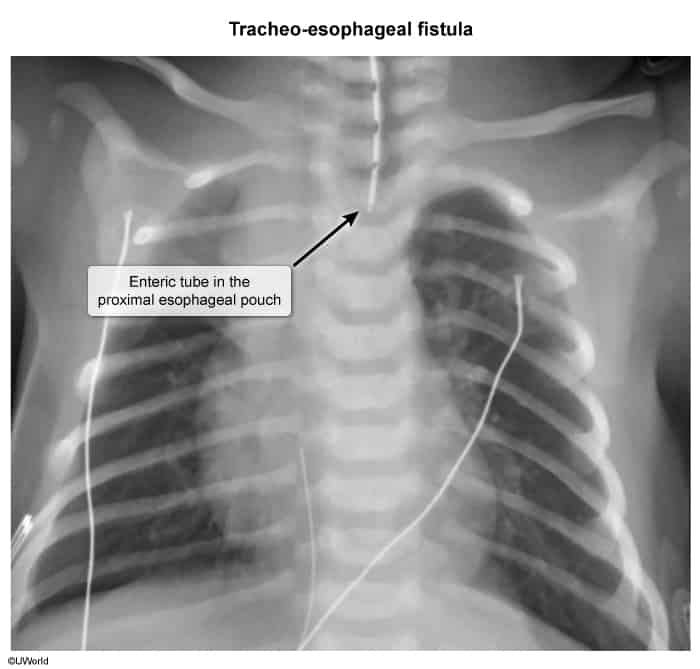
Initial: Attempted passage of NG or OG tube fails (meets resistance at ~10-15 cm).
Imaging: CXR/AXR showing a coiled NG tube in the proximal esophageal pouch. c
Gas-filled GI tract: Confirms distal TEF.
Gasless abdomen: Suggests pure EA or EA w/ proximal TEF only.
Note: Contrast studies are contraindicated due to the high risk of aspiration.
Pre-op Workup: Echocardiogram (to identify aortic arch position for thoracotomy planning and rule out cardiac defects) and renal US (to screen for VACTERL anomalies).
Differential Diagnostics
Choanal atresia: Diff by cyclic cyanosis (worsens during feeding, relieved by crying) and inability to pass catheter through the nose; NG tube easily passes into the stomach.
Laryngomalacia: Diff by inspiratory stridor worsening when supine/crying; feeding is tolerated, and NG tube passes normally.
Duodenal atresia: Diff by bilious vomiting and “double bubble” sign on AXR; no drooling, coughing, or choking immediately upon feeding.
Respiratory Distress Syndrome (RDS): Diff by prematurity, ground-glass CXR pattern, and normal esophageal patency.