All three substances decrease LES tone. Alcohol and caffeine also stimulate gastric acid secretion, which, in combination with frequent TLESRs, increases the risk of esophageal mucosal injury from the gastric refluxate.
GERD is present in up to 80% of pregnancies. The underlying pathophysiology involves increased abdominal pressure, decreased LES tone (due to high estrogen and progesterone levels during pregnancy), and prolonged gastric emptying as a result of reduced gastric motility.
Direct Injury: Microscopic amounts of refluxed acid and pepsin travel up into the throat and airways, causing direct inflammation and irritation.
Vagal Nerve Reflex: Acid in the distal esophagus triggers a nerve reflex (via the vagus nerve) that results in a chronic cough and bronchoconstriction (worsening asthma) without direct aspiration.
Can trigger or worsen asthma.
Alarm features (warrant prompt endoscopy):
Dysphagia (difficulty swallowing) or Odynophagia (painful swallowing).
Unexplained weight loss.
GI bleeding (hematemesis) or iron deficiency anemia.
Diagnostics
Ambulatory 24-hr pH monitoring: Gold standard for confirming abnormal acid reflux, especially if EGD is normal but symptoms persist.
Biopsy
Reflux Esophagitis (Active GERD)
Key Inflammatory Changes:
Scattered intraepithelial eosinophils (most characteristic) and neutrophils.
Basal zone hyperplasia (>15% of epithelial thickness).
Lamina propria papillae elongation (>2/3 of epithelial thickness).
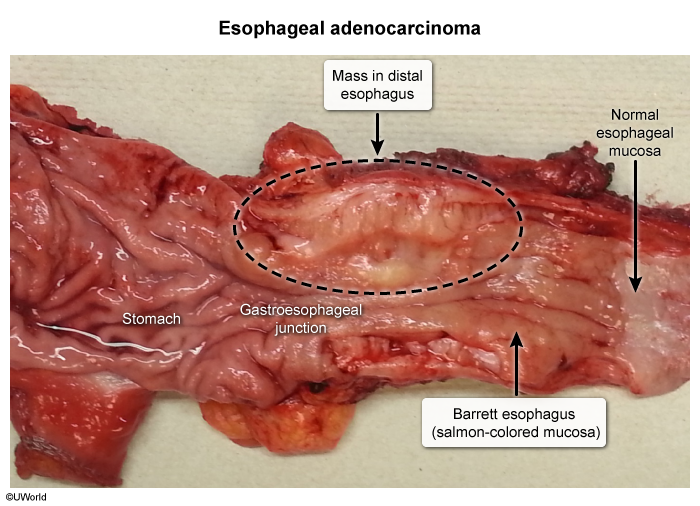
Barrett’s Esophagus (Chronic GERD)
Defining Feature: Intestinal Metaplasia.
Normal squamous epithelium is replaced by columnar epithelium with interspersed goblet cells.
Significance: Precursor to esophageal adenocarcinoma.
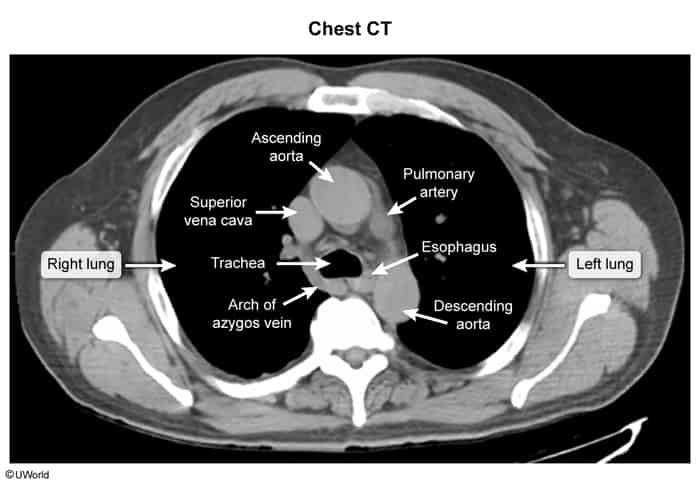
X-ray: the esophagus courses between the trachea and vertebral bodies and is typically collapsed with no visible lumen.
Treatment
Lifestyle/Dietary Modifications: Weight loss, elevating the head of the bed, avoiding meals 2-3 hours before bedtime, and avoiding trigger foods (e.g., fatty/spicy foods, alcohol, caffeine).
Medical Therapy:
Antacids: For rapid, temporary relief of mild, intermittent symptoms.
Magnesium & Aluminum Hydroxide
Combination Rationale: Magnesium hydroxide and aluminum hydroxide are almost always co-formulated. This is done to balance their opposing side effects on bowel motility.
Side Effects:
Aluminum hydroxide: Causes constipation and can lead to hypophosphatemia with chronic use.
Magnesium hydroxide: Causes osmotic diarrhea.
H2-Receptor Antagonists (H2RAs; e.g., Famotidine): For mild GERD.
Proton Pump Inhibitors (PPIs; e.g., Omeprazole, Pantoprazole): First-line for moderate-to-severe symptoms and for healing erosive esophagitis.
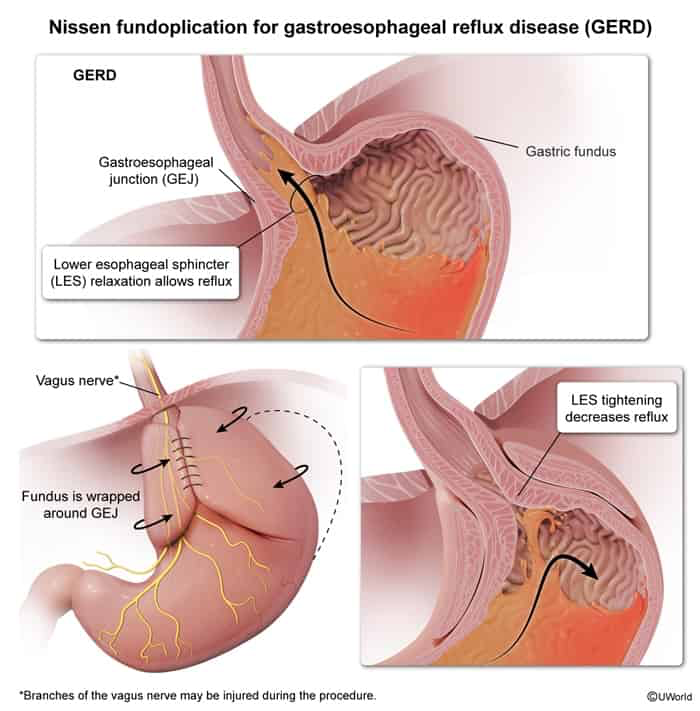
Surgical Tx (Nissen fundoplication): Reserved for patients with refractory symptoms, large hiatal hernias, or those who wish to avoid long-term medical therapy.
Complications
Gas bloat syndrome: inability to belch, leading to bloating and an increase in flatulence
If the stomach is wrapped too tight, LES tone is increased (known as overcorrection) and gas cannot be released orally, but has to leave the body via the intestine.
Vagal Nerve Injury:
Accidental injury during esophageal dissection.
Can cause acute or chronic gastroparesis (early satiety, postprandial nausea/vomiting) or severe diarrhea.
Confirm delayed gastric motility w/ a scintigraphic gastric emptying scan using a radiolabeled solid meal c
Complications
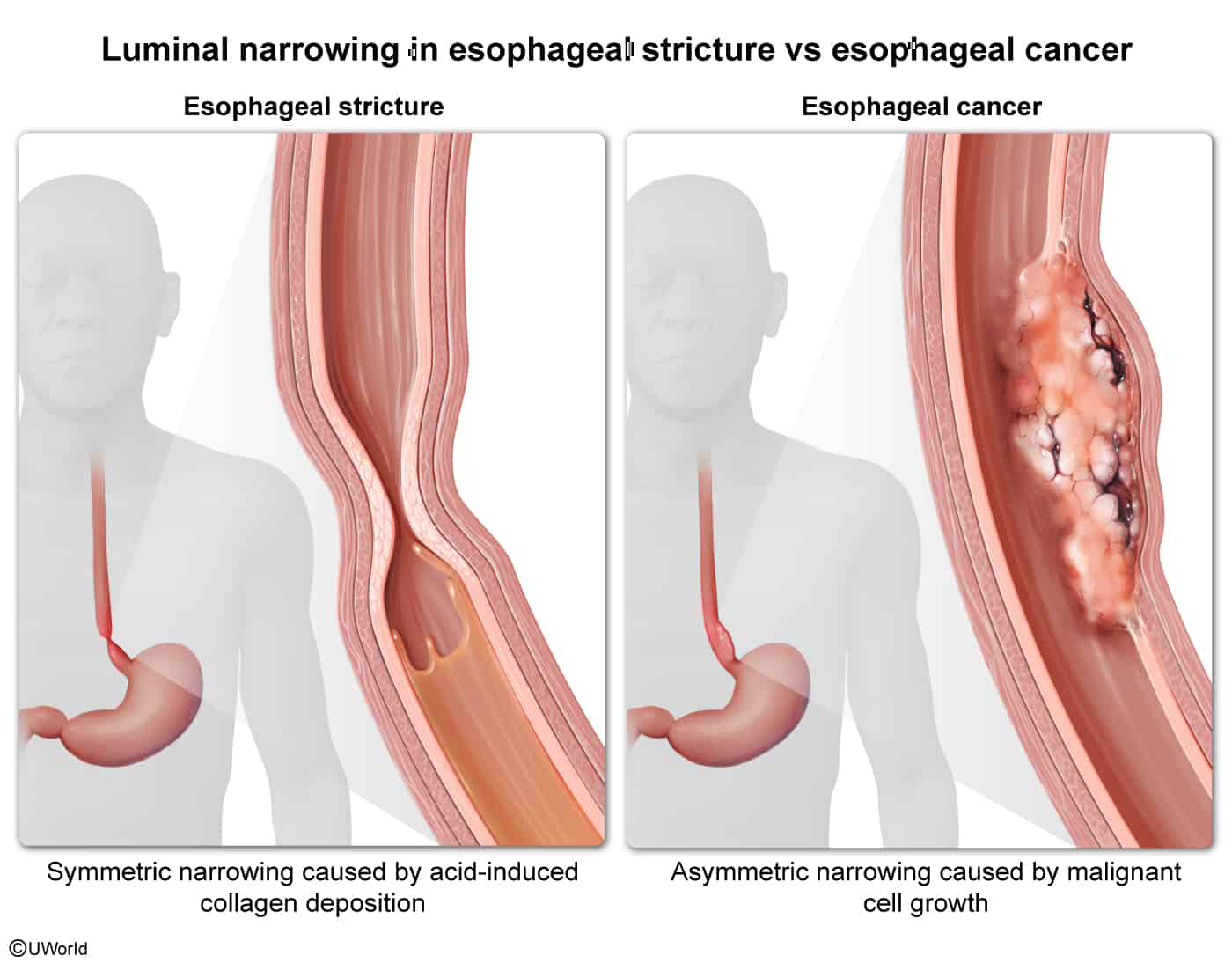
Esophageal Stricture
Epidemiology & Risk Factors
Chronic gastroesophageal reflux disease (GERD) (accounts for >70% of benign peptic strictures).
Caustic ingestion (e.g., household lye, acids).
Radiation therapy (for thoracic or head/neck malignancies).
Key Labs: CBC (may show iron deficiency anemia if chronic occult blood loss or malnutrition) and BMP/albumin (to assess hydration and nutritional status).
Biopsy: Multiple brushings/biopsies from the stricture margin during EGD to exclude dysplasia or carcinoma.
Differential Diagnostics
Esophageal Adenocarcinoma/SCC:
Differentiated by rapid progression of dysphagia, profound weight loss, advanced age, and asymmetric, irregular, or friable mucosal narrowing on barium swallow or EGD.
Achalasia:
Differentiated by concurrent dysphagia to solids AND liquids from the onset, bird’s beak narrowing on barium swallow, and esophageal manometry showing aperistalsis and failure of the LES to relax.
Schatzki Ring:
Differentiated by intermittent (non-progressive) dysphagia to solids (often during a heavy meal, “steakhouse syndrome”). Located at the squamocolumnar junction.
Eosinophilic Esophagitis (EoE):
Differentiated by history of atopy (asthma, eczema, allergies), young male demographic, EGD showing concentric rings (“trachealization”), and mucosal biopsy revealing >15 eosinophils/HPF.
Management
Mechanical Dilation (First-line):
Performed during EGD using balloon dilators or bougies (wire-guided dilators) to physically widen the lumen.
Acid Suppression (First-line adjunct):
High-dose proton pump inhibitor (PPI) therapy (e.g., omeprazole) indefinitely to heal esophagitis and significantly reduce recurrence rates.
Refractory Management:
Intralesional corticosteroid (triamcinolone) injection during dilation to inhibit collagen synthesis.
Temporary placement of self-expanding plastic/metal stents.
Surgical resection (esophagectomy/reconstruction) as a last resort.