Epidemiology
Etiology
- Lax diaphragmatic esophageal hiatus
- Advanced age
- Smoking
- Causes a loss of elastin fibres in the diaphragmatic crura
- Obesity
- Prolonged periods of increased intra-abdominal pressure
- Pregnancy
- Ascites
- Chronic cough
- Chronic constipation
Pathophysiology
Relative negative intrathoracic pressure and the lax hiatus → herniation of the abdominal contents into the thorax → loss of reflux barrier + compromised fluid emptying of distal esophagus → gastroesophageal reflux disease (GERD)
Classification
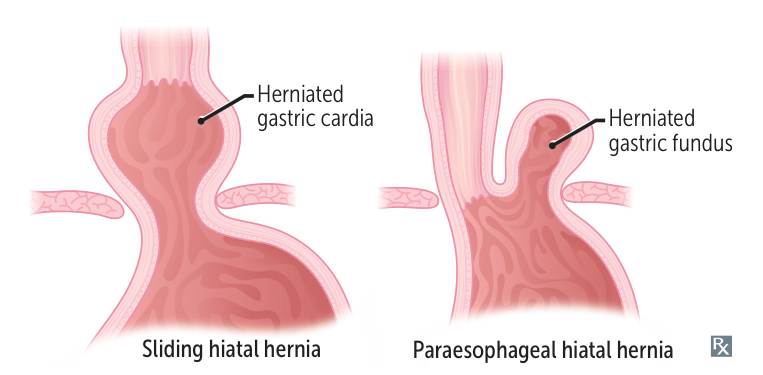
Type I: sliding hiatal hernia
- Most common type (95% of cases)
- The GEJ and the gastric cardia slide up into the posterior mediastinum.
- The gastric fundus remains below the diaphragm (hourglass stomach)
Type II: paraesophageal hiatal hernia
- Part of the gastric fundus herniates into the thorax.
- The GEJ remains in its anatomical position below the diaphragm.
Clinical features
Diagnostics
Treatment
- Type I (Sliding): c
- Lifestyle: Weight loss, small frequent meals, avoid late meals, elevate head of bed.
- Medical: PPI (first-line), H2 blockers (alternative).
- Surgical (Nissen fundoplication): Indications = refractory GERD despite max medical Rx, complications (stricture, Barrett’s, recurrent aspiration).
- Type II-IV (Paraesophageal):
- Asymptomatic/Minimal symptoms: Conservative vs elective repair (debated; trend toward repair if fit).
- Symptomatic (anemia, dysphagia): Elective laparoscopic repair.
- Emergent (volvulus/strangulation): Immediate surgical reduction + gastropexy ± gastrectomy if necrosis.