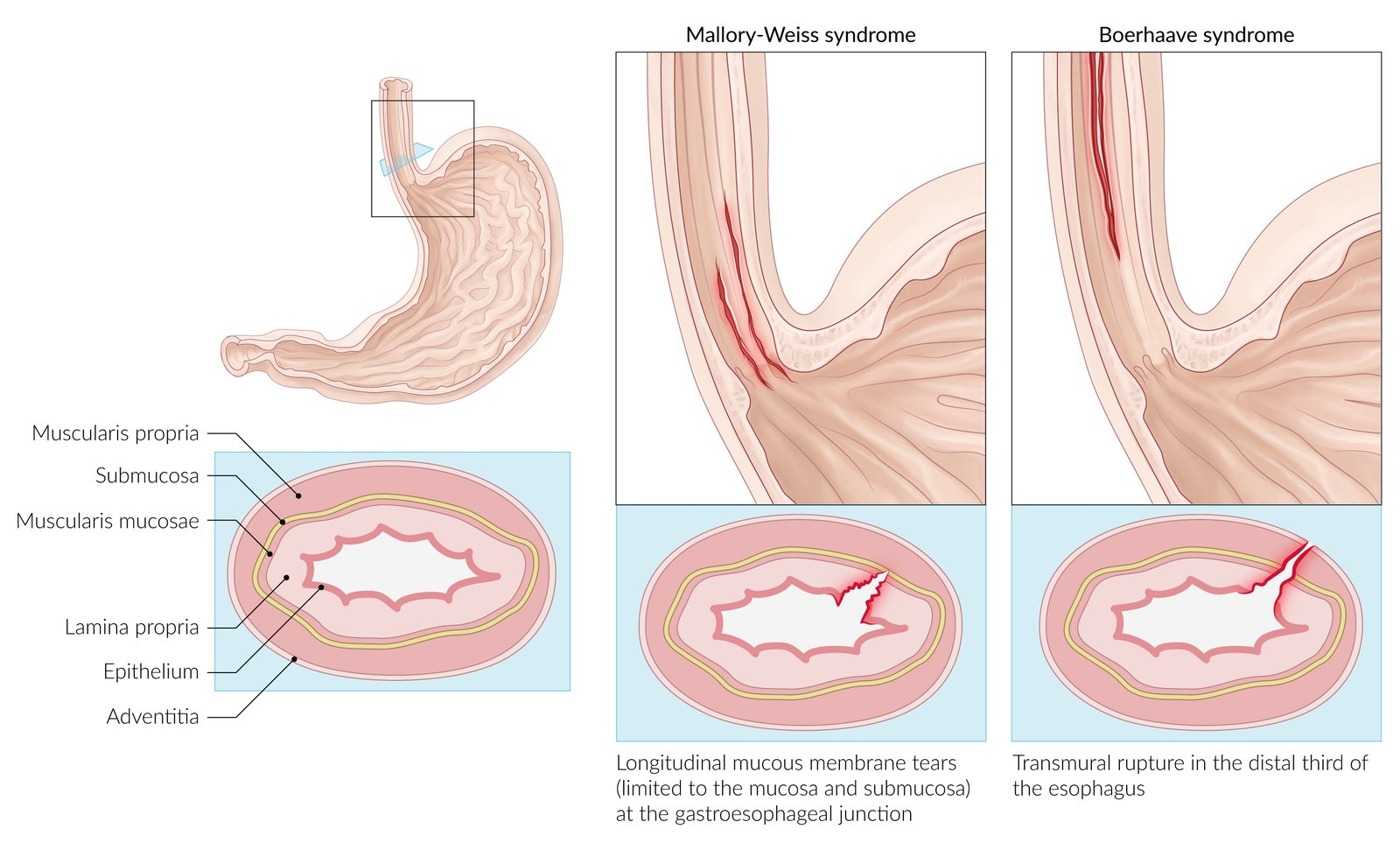
Mechanism: a sudden and severe rise in the esophageal intraluminal pressure results in tearing of the esophageal mucous membrane, as well as the submucosal arteries and veins
Often a single longitudinal tear (but multiple tears are possible) in the mucosa at the gastroesophageal junction or in the cardia of the stomach which are limited to the mucosa and submucosa
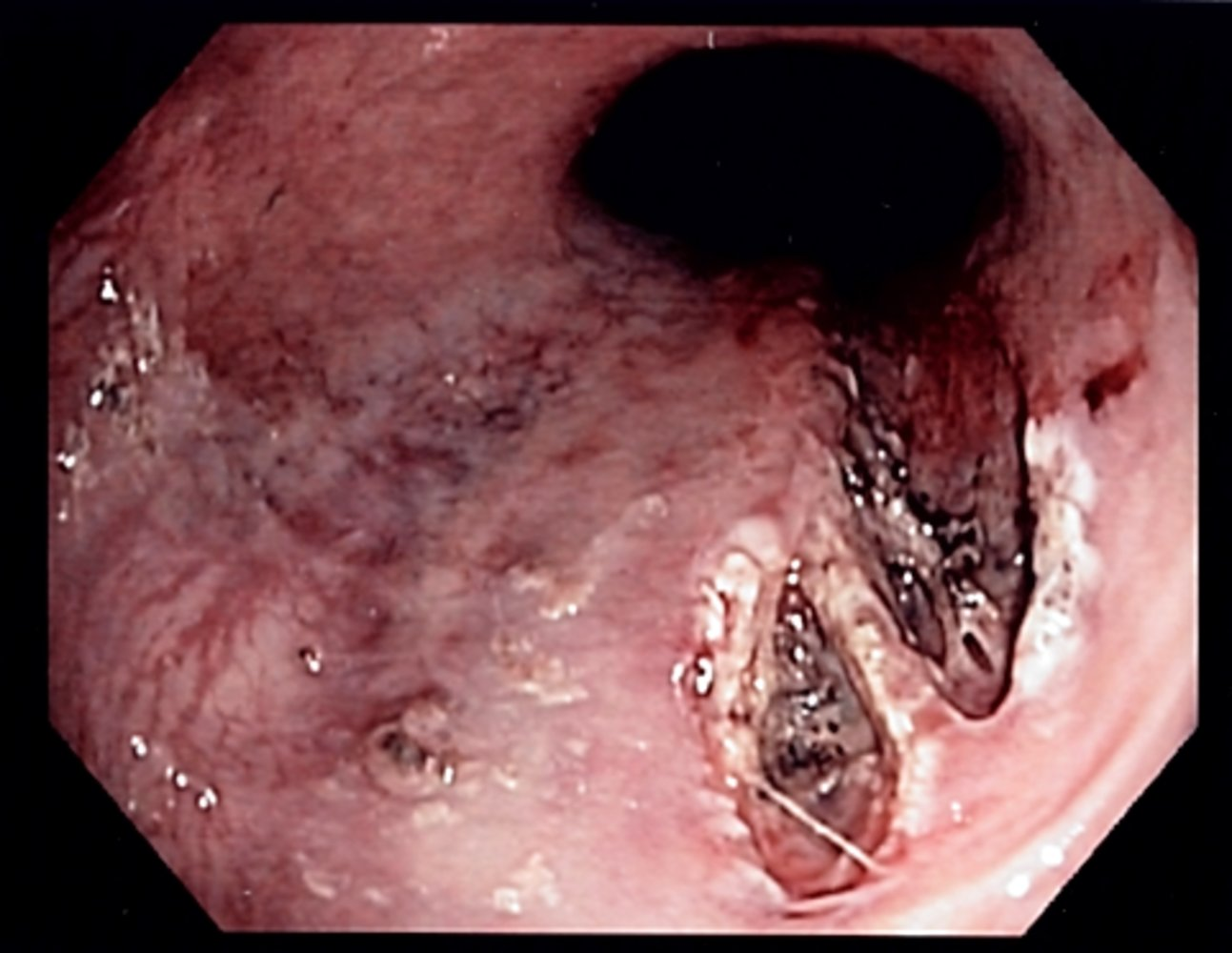
A fibrin crust over the split, a clot, or active bleeding may be evident.