Etiology
- Risk factors for asthma include:
- Family history of asthma
- Past history of allergies
- Atopic dermatitis
- Low socioeconomic status
- Allergic asthma (extrinsic asthma) vs Nonallergic asthma (intrinsic asthma)
- Allergic asthma (extrinsic asthma)
- Cardinal risk factor: atopy
- Environmental allergens: pollen (seasonal), dust mites, domestic animals, mold spores
- Allergic occupational asthma from exposure to allergens in the workplace (e.g., flour dust)
- Nonallergic asthma (intrinsic asthma)
- Viral respiratory tract infections (one of the most common stimuli, especially in children)
- Cold air
- Physical exertion (laughter, exercise-induced asthma)
- Gastroesophageal reflux disease (GERD): often exists concurrently with asthma
- Chronic sinusitis or rhinitis
- Medication: aspirin/NSAIDS (aspirin-induced asthma), beta blockers
- Stress
- Irritant-induced occupational asthma (e.g., from exposure to solvents, ozone, tobacco or wood smoke, cleaning agents)
- Allergic asthma (extrinsic asthma)
Tip
- Allergic asthma (extrinsic asthma): A type of asthma triggered by allergens (e.g., pollen, dust mites, mold spores, pet allergens). Typically onset in childhood.
- Nonallergic asthma (intrinsic asthma): A type of asthma that typically develops in patients > 40 years of age.
Pathophysiology
Common underlying pathophysiology
- Core Pathophysiology
- Chronic disorder of airway hyperresponsiveness, inflammation, and reversible bronchoconstriction.
- Symptoms are primarily caused by inflammation of the terminal bronchioles, which are lined with smooth muscle but lack the cartilage found in larger airways.
- Key Cells: Eosinophils, Mast Cells, Th2 lymphocytes.
- Airflow: ↓ FEV1/FVC ratio, reversible with bronchodilators.
- Chronic disorder of airway hyperresponsiveness, inflammation, and reversible bronchoconstriction.
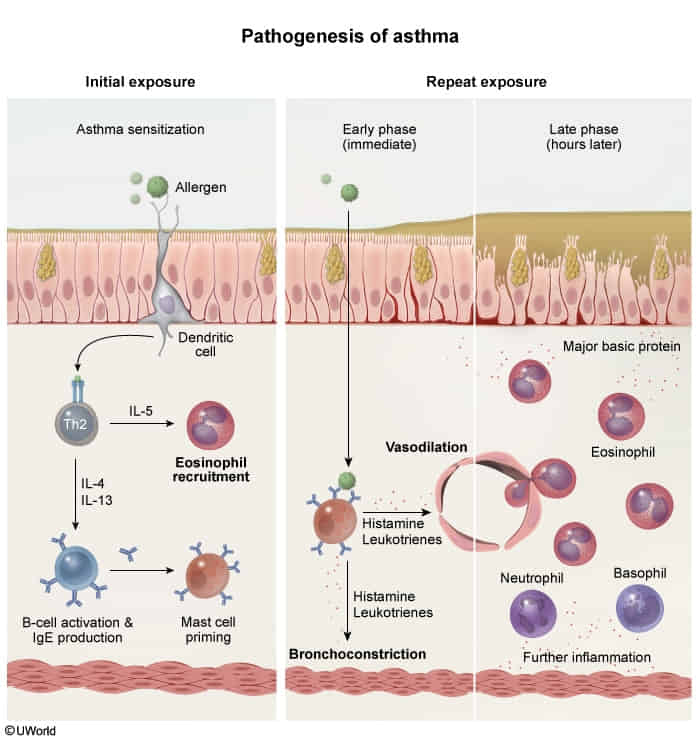
- Allergic (Extrinsic) Asthma
- Type I Hypersensitivity Reaction (most common type).
- Mechanism: Allergen exposure → APC presents to Th2 cell → Th2 secretes:
- IL-4/IL-13: Stimulates B-cells to produce IgE.
- IL-5: Recruits and activates eosinophils.
- Action: IgE coats mast cells. Re-exposure → mast cell degranulation → release of histamine & leukotrienes → bronchospasm.
- Late Phase: Eosinophil-mediated inflammation damages epithelium.
- Non-Allergic (Intrinsic) Asthma
- Triggers: Viral infections (RSV, rhinovirus), cold air, stress.
- Mechanism: Not IgE-mediated. Normal serum IgE. Inflammation is driven by non-atopic stimuli.
- Iirritant enters lung → ↑ release of neutrophils → submucosal edema → airway obstruction
- Aspirin-Exacerbated Respiratory Disease (AERD)
- Samter’s Triad: Asthma + Nasal Polyps + Aspirin/NSAID sensitivity.
- Mechanism: NSAID inhibition of COX pathway shunts arachidonic acid to the lipoxygenase pathway → ↑ Leukotrienes → severe bronchoconstriction.
- Classic Pathology Findings
- Curschmann spirals: Whorled mucus plugs.
- Charcot-Leyden crystals: Crystalline breakdown products of eosinophils.
- Airway Remodeling (Chronic): Smooth muscle hypertrophy and sub-basement membrane fibrosis.
Clinical features
Subtypes and variants
- Allergic asthma
- Most common phenotype
- Begins with intermittent symptoms in childhood
- Triggered by allergens
- Usually associated with atopy (e.g., eczema, rhinitis)
- Responds well to ICS-containing treatment
- Nonallergic asthma
- Less common than allergic asthma
- Triggered by, e.g., viral upper respiratory tract infections, cold air, GERD
- Not associated with atopy
- Responds poorly to ICS-containing treatment
- Cough variant asthma: a type of asthma characterized by chronic dry cough without other typical symptoms of asthma
- Cough often worsens at night.
- Aspirin-exacerbated respiratory disease
- Occupational asthma
- Diagnosis
- Initial/Screening: Serial Peak Expiratory Flow (PEF) monitoring (logging values at work vs. days off) for 2–4 weeks.
- Key Labs/Imaging: Baseline spirometry demonstrating reversible airflow obstruction (FEV1/FVC < 0.70; ↑ FEV1 by >12% and >200 mL post-bronchodilator).
- Confirmatory/Gold Standard: Specific Inhalation Challenge (SIC) with the suspected workplace agent (often reserved for specialized centers).
- Alternative Testing: Methacholine challenge test (high negative predictive value to rule out asthma if spirometry is normal). Skin prick/serum specific IgE testing for HMW agents.
- Diagnosis
- Asthma in pregnancy
- Risk factors
- Severe asthma prior to pregnancy
- Obesity & excessive first-trimester weight gain
- Smoking during pregnancy
- Asthma symptoms may be worse, better, or unchanged during pregnancy.
- Same stepwise management as with other patients
- Inhalation treatments preferred
- Poorly managed asthma can increase the risk of pregnancy complications (e.g., preeclampsia, premature birth, congenital abnormalities).
- Monthly monitoring of asthma is recommended.
- Risk factors
Differential diagnostics
| Feature | Cardiogenic “Asthma” (Heart Failure) | Bronchial Asthma |
|---|---|---|
| Pathophysiology | LV failure → pulmonary edema → airway narrowing. | Airway inflammation (IgE/eosinophilic) → bronchoconstriction. |
| Patient Profile | Older patient, history of CHF, HTN, MI. | Younger patient, history of atopy (eczema, allergies). |
| Key Symptoms | Orthopnea, PND, pink frothy sputum. | Nocturnal cough, triggered by allergens/exercise. |
| Physical Exam | JVD, S3 gallop, bibasilar crackles/rales. | Diffuse expiratory wheezing, often normal between exacerbations. |
| Key Diagnostics | ↑ BNP, Kerley B lines & cardiomegaly on CXR. | PFTs show reversible obstruction post-bronchodilator. |
| Management | Diuretics (e.g., Furosemide), Nitrates, O2, BiPAP. | Bronchodilators (e.g., Albuterol), Corticosteroids. |
Diagnostics
Spirometry
- Supportive findings: Expiratory airway limitation: i.e., ↓ FEV1 and ↓ FEV1/FVC ratio
- Bronchodilator Responsiveness Testing:
- Used when the patient has abnormal baseline spirometry showing obstruction (FEV1/FVC ≤70%)
- Tests if the obstruction is reversible (suggesting asthma) or fixed (suggesting conditions like COPD)
- Not useful if current spirometry is normal, even if the patient has asthma symptoms
- Quick test: perform spirometry → give bronchodilator → repeat spirometry
- Bronchial Challenge Testing:
- Identify airway hyperresponsiveness and bronchoconstriction in response to direct, nonallergic stimuli (e.g., methacholine, histamine) or indirect stimuli (e.g., exercise, hyperventilation).
- Used when patient has symptoms suggestive of asthma but normal baseline spirometry
- Tests for airway hyperresponsiveness by attempting to provoke bronchospasm
- Particularly useful for patients with intermittent symptoms who are asymptomatic during office visits
- More time-intensive: involves giving increasing doses of the provocative agent and measuring response
Allergen Testing
- Sensitization vs. Allergy: A (+) Skin Prick Testing (SPT) or Serum Specific IgE (sIgE) only indicates sensitization. Diagnosis of allergy requires (+) test AND clinical symptoms on exposure. c
Treatment
Approach
1. Chronic Asthma Management (Stepwise)
- Prerequisite: Assess adherence and inhaler technique before stepping up therapy.
- Step 1 (Intermittent): Symptoms < 2 days/week, nighttime awakenings 2x/month.
- Preferred (GINA Track 1): As-needed low-dose ICS-formoterol.
- Alternative (Track 2): As-needed SABA + low-dose ICS whenever SABA is taken.
- Step 2 (Mild Persistent): Symptoms > 2 days/week (but not daily), nighttime awakenings 3-4x/month.
- Preferred: Daily low-dose ICS + as-needed SABA, OR as-needed low-dose ICS-formoterol.
- Alternative: LTRA (montelukast).
- Step 3 (Moderate Persistent): Symptoms daily, nighttime awakenings > 1x/week (not nightly).
- Preferred: Daily low-dose ICS-LABA + as-needed SABA, OR low-dose ICS-formoterol as SMART (Single Maintenance and Reliever Therapy).
- Step 4 (Severe Persistent): Symptoms throughout the day, nighttime awakenings nightly.
- Preferred: Daily medium-dose ICS-LABA as SMART or maintenance + SABA reliever.
- Alternatives: Add LAMA (tiotropium) or LTRA.
- Step 5: High-dose ICS-LABA + phenotypic assessment for biologic therapies (e.g., omalizumab [anti-IgE], mepolizumab [anti-IL-5]).
- Refractory: Low-dose oral corticosteroids (OCS) (minimize use due to systemic adverse effects).
2. Acute Asthma Exacerbation
- Oxygen: Maintain 93-95% (92-95% in pregnancy).
- Bronchodilators: Inhaled SABA (albuterol) + SAMA (ipratropium) nebulizers every 20 mins or continuously for the first hour.
- Systemic Corticosteroids: IV methylprednisolone or PO prednisone (give early; takes 4-6 hours to work).
- Refractory (Severe): IV (single dose, induces smooth muscle relaxation).
- Intubation & Mechanical Ventilation:
- Critical Exam Indicator: Normalization of on ABG (or rising ) in a tachypneic patient. Indicates respiratory muscle fatigue and impending respiratory failure. c
- Other indications: Silent chest on auscultation (no air movement), altered mental status.
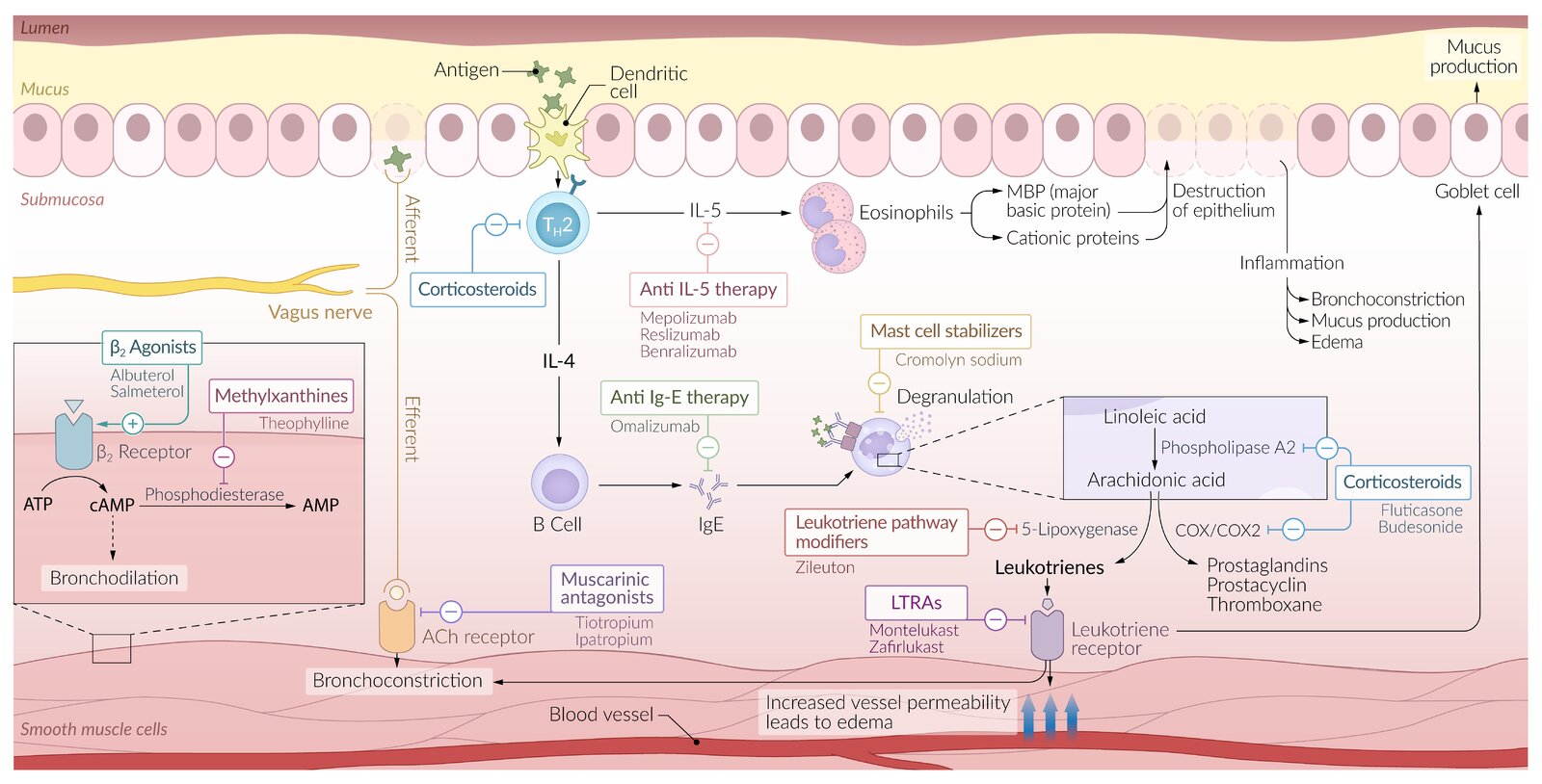
Antileukotrienes
Leukotriene receptor antagonists (LTRAs)
- Montelukast, Zafirlukast
- Uses
- Exercise-induced
- Prevent leukotrienes from binding to their receptors (CysLT1)→ ↓ bronchoconstriction and inflammation
- Asthma aspirin-induced asthma
- Long-term maintenance treatment (particularly in children)
Leukotriene pathway modifiers
- Zileuton
- Inhibit 5-lipoxygenase → ↓ production of leukotrienes → ↓ bronchoconstriction and inflammation
- Uses
- Exercise-induced asthma
- Aspirin-induced asthma
Mnemonic
Antileukotrienes -> Montelukast, zafirlukast, zileuton
Long-acting muscarinic antagonists (LAMA)
- Tiotropium bromide(噻托溴铵)
- Long-term maintenance treatment
Mast cell stabilizers (chromones)
- Cromolyn
- Inhibit mast cell degranulation and prevent release of preformed chemical mediators.
- Uses
- Preventive treatment prior to exercise
Biologics
Anti-IgE antibodies
- Omalizumab 单抗记忆
- Binds to serum IgE → ↓ expression of high-affinity IgE receptors (FcεRI) on mast cells and basophils
- Uses
- Select cases of severe asthma
IL-5 antibodies
- mepolizumab, reslizumab,benralizumab
- Block the effects of IL-5 on eosinophils → ↓ chemotaxis and ↓ cell differentiation, maturation, and activation
- Uses
- Refractory severe eosinophilic asthma