Acute Bleeding: IV Octreotide (splanchnic vasoconstriction) + Ceftriaxone (prophylaxis against SBP) + urgent EGD (within 12 hours) for EVL.
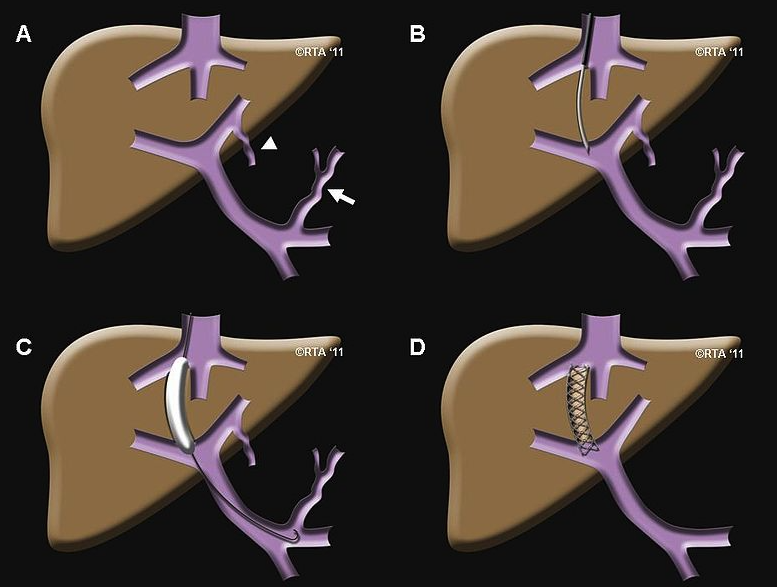
Refractory Bleeding: TIPS.
Hepatic Encephalopathy:
First-line: Lactulose (titrate to 2-3 soft stools/day to convert ammonia to non-absorbable ammonium).
Second-line (or add-on for recurrent episodes): Rifaximin (decreases ammonia-producing gut bacteria).
HCC Screening:
RUQ US +/- AFP every 6 months for all cirrhotic patients. c
Complications
Complications screening
Hepatocellular Carcinoma (HCC) Surveillance
Indication: All pts with Child-Pugh Class A or B cirrhosis. Pts with Child-Pugh Class Conly if they are listed for liver transplantation (otherwise, surveillance does not improve survival).
Modalities: Abdominal ultrasound (US) AND serum alpha-fetoprotein (AFP).
Frequency: Every 6 months.
Management of abnormal screen:
Nodule ≥ 1 cm: Order diagnostic multiphase contrast-enhanced CT or MRI of the liver (LI-RADS protocol showing arterial enhancement with venous washout).
Nodule < 1 cm: Repeat US and AFP in 3–6 months.
Elevated AFP with normal/inconclusive US: Order diagnostic multiphase CT or MRI.
Gastroesophageal Varices Screening
Indication: All pts at the time of initial diagnosis of cirrhosis. c
Alternative (Baveno Criteria): Screening EGD can be deferred if liver stiffness measurement (LSM) by transient elastography is < 20 kPa AND platelet count is > 150,000/µL.
Surveillance Intervals (by EGD findings):
No varices: EGD every 2–3 years if compensated; annually if decompensated.
Small varices: EGD every 1–2 years if compensated; annually if decompensated. Start non-selective beta-blockers (NSBB) (e.g., carvedilol, nadolol, propranolol) if high risk of bleeding (e.g., red wale signs, Child-Pugh C).
Medium/Large varices: Do not repeat screening EGD. Initiate primary prophylaxis immediately with NSBB or endoscopic variceal ligation (EVL).
Osteoporosis Screening
Rationale: Pts with cirrhosis have high risk of hepatic osteodystrophy (due to Vitamin D deficiency, malnutrition, and direct inflammatory bone resorption).
Frequency: Baseline at diagnosis. Repeat every 2–3 years if normal.
Preventative Care & Vaccinations
Immunizations:
Hepatitis A & B (if seronegative/non-immune).
Pneumococcal vaccine (PCV20 or PCV15 followed by PPSV23).
Annual influenza vaccine.
Substance Avoidance:
NSAIDs: Absolutely contraindicated (inhibits renal prostaglandins, leading to renal vasoconstriction and precipitating AKI/hepatorenal syndrome).
Alcohol: Complete cessation.
Acetaminophen: Limit to < 2 g/day.
Portal hypertension
Portal-Caval Anastomoses
These are connections between the portal venous system and the systemic (caval) venous system. In portal hypertension, these sites become engorged and dilated as blood is shunted away from the high-pressure liver.
Esophageal:
Portal: Left Gastric Vein
Caval: Esophageal branches of the Azygos Vein (drains to SVC)
Clinical:Esophageal Varices (risk of life-threatening hematemesis).
Portal: Veins draining the ascending/descending colon, spleen, and liver.
Caval: Veins of the posterior abdominal/body wall (e.g., renal, lumbar veins).
Clinical: Usually asymptomatic, but can be a source of occult bleeding.
Management/Treatment
Treatment is aimed at managing and preventing life-threatening complications.
Primary Prophylaxis of Variceal Bleeding:
Non-selective β-blockers (e.g., propranolol, nadolol): Decrease portal pressure by reducing cardiac output and causing splanchnic vasoconstriction. c
Endoscopic Variceal Ligation (EVL): Banding of varices to prevent rupture.
Acute Variceal Bleeding:
Medical Emergency: Secure airway, resuscitate with fluids/blood products.
Octreotide (somatostatin analog): Causes splanchnic vasoconstriction, reducing portal flow. c
Urgent EGD: For banding/ligation of bleeding varices. Perform within 12 hours of presentation once hemodynamically stable.
Refractory Bleeding/Ascites:
Transjugular Intrahepatic Portosystemic Shunt (TIPS): A stent placed between the portal vein and hepatic vein, shunting blood to decompress the portal system. Risk of worsening hepatic encephalopathy.
Ascites Management: Sodium restriction, diuretics (spironolactone, furosemide), and paracentesis for large volumes.
Definitive Treatment: Liver transplantation for end-stage liver disease.
Pulmonary complications of cirrhosis
Hepatic hydrothorax
Definition: pleural effusions (typically one-sided; 70% right, 18% left) with transudate characteristics in the absence of any other cardiac, pulmonary, or pleural disease
Pathophysiology: increased permeability of the diaphragm (small defects, increased abdominal pressure)