Epidemiology
Etiology
Diarrhea is classified by mechanism (secretory, osmotic, inflammatory) or duration (acute <2 wks, persistent 2-4 wks, chronic >4 wks). Stool characteristics and patient history are key to diagnosis.
| Feature | Non-Inflammatory Diarrhea | Inflammatory Diarrhea (Dysentery) |
|---|---|---|
| Pathology | No mucosal invasion; toxin-mediated | Mucosal invasion & destruction |
| Location | Small Bowel | Colon |
| Stool Volume | Large | Small, frequent |
| Stool Content | Watery | Bloody, mucoid (pus) |
| Fever | Usually absent | Common |
| Fecal WBCs | No WBCs t | Present |
| Key Symptom | Dehydration | Tenesmus, severe abd pain |
| Example Bugs | V. cholerae, ETEC, Norovirus, Giardia | Shigella, Campylobacter, EHEC, Salmonella |
Stool Osmotic Gap (SOG)
- Crucial tool to differentiate osmotic from secretory diarrhea.
- Formula:
- Key interpretations:
- SOG < 50 mOsm/kg: Secretory diarrhea (electrolytes account for stool osmolality).
- SOG > 100 mOsm/kg: Osmotic diarrhea (non-absorbable solutes account for stool osmolality).
Secretory Diarrhea
- Pathophysiology: Active secretion of electrolytes (mainly via CFTR or cAMP-mediated pathways) or inhibition of active sodium absorption.
- Clinical Presentation:
- Large volume (> 1 L/day) watery diarrhea.
- Persists during fasting or sleep (no change in stool volume). c
- SOG < 50 mOsm/kg.
- High-Yield Etiologies:
- Infectious: Vibrio cholerae, ETEC (heat-labile/stable toxins activate adenylate/guanylate cyclase).
- Hormonal/Neuroendocrine: VIPoma (WDHA syndrome: watery diarrhea, hypokalemia, achlorhydria), Carcinoid syndrome (flushing, bronchospasm, tricuspid regurgitation), Gastrinoma (Zollinger-Ellison).
- Malabsorption: Unabsorbed bile acids (post-ileal resection; stimulates colonic secretion). c
- Inflammatory: Microscopic colitis (collagenous or lymphocytic).
Osmotic Diarrhea
- Pathophysiology: Ingestion or accumulation of non-absorbable, osmotically active solutes in the intestinal lumen that draw water out of enterocytes.
- Clinical Presentation:
- Improves or resolves with fasting (or when oral intake of the offending agent ceases).
- SOG > 100 mOsm/kg.
- Stool pH is often acidic (< 5.5) in carbohydrate malabsorption due to bacterial fermentation.
- High-Yield Etiologies:
- Carbohydrate Malabsorption: Lactose intolerance (lactase deficiency), fructose or sorbitol/xylitol ingestion (sugar-free gum/candies).
- Laxative Abuse: Magnesium-containing laxatives, polyethylene glycol (PEG), lactulose.
- Mucosal Malabsorption: Early-stage Celiac disease or tropical sprue.
Inflammatory (Exudative) Diarrhea
- Pathophysiology: Mucosal invasion or inflammation leading to cell death, ulceration, and disruption of tight junctions, causing exudation of mucus, blood, and proteins.
- Clinical Presentation:
- Fever, systemic symptoms, severe abdominal cramping, and tenesmus.
- Small volume, frequent, bloody stools (dysentery).
- Presence of fecal leukocytes, lactoferrin, or fecal calprotectin.
- High-Yield Etiologies:
- Infectious (Invasive): Shigella, Salmonella, Campylobacter jejuni, Yersinia enterocolitica, EIEC, EHEC (O157:H7; risk of HUS with Abx), Clostridioides difficile, Entamoeba histolytica.
- Non-Infectious: Inflammatory Bowel Disease (IBD - Crohn disease and Ulcerative Colitis), radiation colitis, ischemic colitis.
Malabsorptive (Fatty) Diarrhea
- Pathophysiology: Impaired digestion (maldigestion) or mucosal absorption (malabsorption) of dietary fats and nutrients.
- Clinical Presentation:
- Steatorrhea: Foul-smelling, greasy, pale, bulky stools that float and are difficult to flush.
- Significant weight loss, muscle wasting, and nutritional deficiencies.
- Deficiencies in fat-soluble vitamins (A, D, E, K):
- Vitamin A: Night blindness, dry skin.
- Vitamin D: Osteomalacia, hypocalcemia.
- Vitamin E: Ataxia, hemolytic anemia.
- Vitamin K: Easy bruising, elevated PT/INR.
- High-Yield Etiologies:
- Maldigestion (Luminal Phase): Chronic pancreatitis (alcohol abuse, cystic fibrosis; exocrine pancreatic insufficiency), bile acid deficiency (due to terminal ileal resection or biliary obstruction).
- Malabsorption (Mucosal Phase):
- Celiac disease (anti-tTG IgA, intraepithelial lymphocytosis, villous atrophy).
- Crohn disease (terminal ileum involvement).
- Whipple disease (Tropheryma whipplei; PAS-positive macrophages in lamina propria, arthralgias, neurological symptoms).
- Small Intestinal Bacterial Overgrowth (SIBO; premature deconjugation of bile acids).
Motility-Related (Functional) Diarrhea
- Pathophysiology: Altered gut motility leading to rapid intestinal transit time, leaving insufficient time for adequate absorption of water and nutrients.
- Clinical Presentation:
- Highly variable, postprandial urgency, often alternating with constipation.
- No systemic symptoms, normal nocturnal bowel habits (no diarrhea wakes pt up from sleep).
- Normal labs (normal CBC, ESR/CRP, SOG).
- High-Yield Etiologies:
- Irritable Bowel Syndrome (IBS-D): Chronic abdominal pain relieved by defecation, associated with change in stool frequency/form.
- Endocrine: Hyperthyroidism (thyrotoxicosis; increased sympathetic drive).
- Neuropathic: Diabetic enteropathy (autonomic neuropathy).
- Surgical: Post-vagotomy or post-gastrectomy dumping syndrome (hyperosmolar load into duodenum leads to rapid fluid shifts and transit).
Pathophysiology
Inflammatory
- EHEC
- Shiga-like toxin: bloody diarrhea
- Enhanced cytokine release (mainly renal epithelial cells) → HUS (no invasion of host cells)
- Shigella
- Spread from cell to cell → invasion of M cells (MALT)
- Shiga toxin
- Campylobacter
- Type IV secretion system (T4SS)
- Cytolethal-distending toxin
- Non-Typhi Samonella
- Flagellar motility
- Endotoxin
- Clostridioides difficile
- Toxin A (enterotoxin)
- Toxin B (cytotoxin)
- Yersinia Enterocolitica
- Amebic Dysentery
- Vibrio parahaemolyticus/vulnificus
Noninflammatory
- ETEC
- Heat-labile toxin
- Overactivates adenylate cyclase → ↑ cAMP → ↑ secretion of chloride and water efflux into the intestinal lumen → watery diarrhea
- Heat-stable toxin
- Activation of guanylate cyclase → ↑ cGMP → ↓ NaCl reabsorption → water efflux into the intestinal lumen → secretory diarrhea
- Heat-labile toxin
- V. cholerae
- Cholera toxin (enterotoxin): “rice-water” diarrhea
- Same with heat-labile toxin
- Permanently activates Gs protein → overactivation of adenylate cyclase → ↑ cAMP → ↑ secretion of chloride and water efflux into the intestinal lumen → watery diarrhea.
- Cholera toxin (enterotoxin): “rice-water” diarrhea
- Giardiasis
- Impaired function and structure of intestinal tissue, resulting in malabsorption and diarrhea
- Gastroenteritis from preformed enterotoxin (S. aureus, B. cereus)
- See Food poisoning
- S. aureus: Enterotoxin B
- Forms pores in enterocyte membranes → leakage of Na+ and water into the intestinal lumen
- C. perfringens
- Exotoxins
- Clostridium perfringens alpha toxin
- Acts as a phospholipase → degrades cell membranes and tissue.
- Enterotoxin (heat-labile)
- Responsible for food poisoning.
- Cryptosporidiosis
- Norovirus
- Rotavirus
Clinical features
Diagnostics
Subtypes and variants
Factitious Diarrhea (Laxative Abuse)
- Epidemiology: Typically females, healthcare workers, or pts w/ psychiatric Hx (e.g., factitious disorder).
- Etiology: Surreptitious self-administration of laxatives (e.g., bisacodyl, senna, magnesium) or dilution of stool w/ water.
- Clinical Features:
- Chronic, watery, nocturnal diarrhea (distinguishes from functional diarrhea/IBS).
- Volume depletion (orthostasis, tachycardia).
- Diagnostic Workup:
- Stool Osmotic Gap = 290 - 2 * (Stool [Na+] + Stool [K+]).
- Gap < 50 mOsm/kg: Secretory diarrhea (stimulants: bisacodyl, senna).
- Gap > 100 mOsm/kg: Osmotic diarrhea (osmotic laxatives: Mg2+, phosphate).
- Stool Osmolality < 250 mOsm/kg: Suggests stool dilution w/ water.
- Confirmatory: Urine/stool laxative screen or elevated stool Mg2+ levels.
- Endoscopy: Melanosis coli: Dark brown pigmentation of colonic mucosa w/ pale lymphoid follicles (anthraquinone/senna use). c
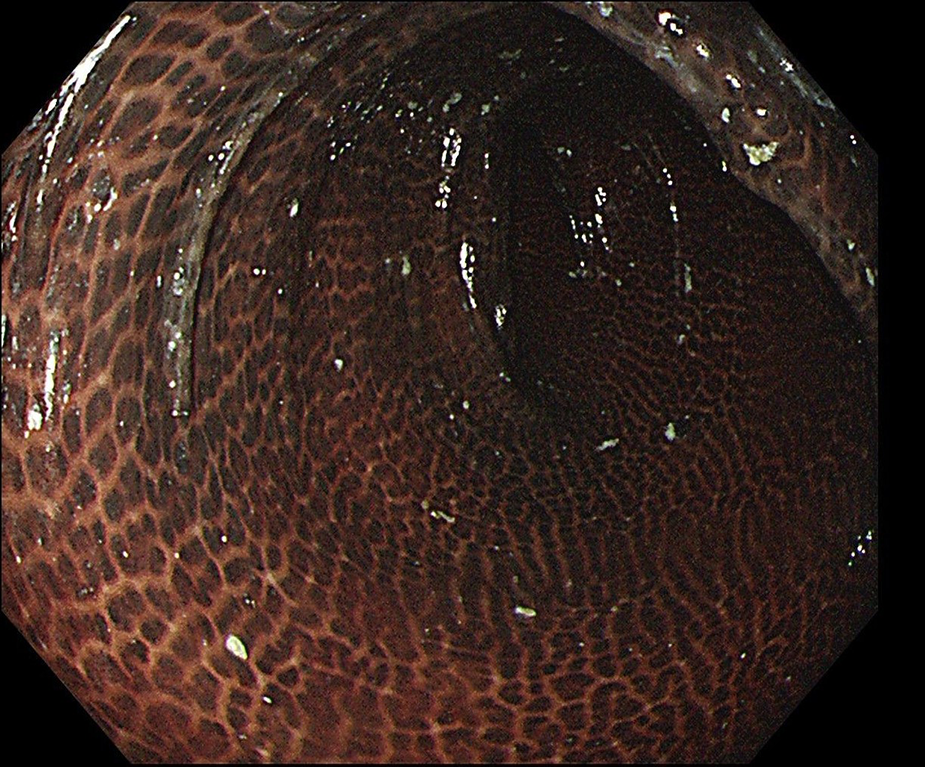
- Apoptosis: Anthraquinones (e.g., senna) damage colonocytes -> trigger mass apoptosis.
- Pigmentation: Lamina propria macrophages engulf apoptotic cells -> degrade them to lipofuscin (brown-black pigment, not melanin).
- Sparing: Lymph follicles (and adenomatous polyps) lack these phagocytic macrophages -> remain pale.
- Stool Osmotic Gap = 290 - 2 * (Stool [Na+] + Stool [K+]).
- Management:
- Stabilize w/ IVF and correct severe hypokalemia/electrolytes.
- Implement non-judgmental psych referral; avoid aggressive, hostile confrontation.
- Complications: Hypokalemia (cardiac arrhythmias), metabolic acidosis, and AKI.
Bile acid diarrhea
- Definition: secretory diarrhea with or without steatorrhea due to increased colonic secretion and motility secondary to an increased concentration of bile acids within the colon
- Etiology
- Crohn disease (CD): Terminal ileitis impairs enterohepatic circulation of bile acids.
- Ileal resection:
- Resection < 100 cm: Moderate malabsorption leads to watery, secretory diarrhea (bile acid spillover to colon).
- Resection > 100 cm: Severe malabsorption depletes the bile acid pool, resulting in fat malabsorption and steatorrhea.
- Cholecystectomy: Loss of gallbladder storage leads to constant biliary drainage into the intestine. c
- Small Intestinal Bacterial Overgrowth (SIBO): Bacterial deconjugation of bile acids impairs absorption.
- Idiopathic (Primary) BAD: Deficient FGF-19 feedback results in hepatic hyper-synthesis of bile acids.
- Clinical features
- Chronic watery diarrhea: Classic secretory pattern (frequent, large-volume, occurs at night, and does not improve with fasting).
- Urgency, bloating, and fecal incontinence.
- Steatorrhea: Greasy, foul-smelling, floating stools (typically seen only in extensive terminal ileal resections > 100 cm).
- Management
- First-line:
- Bile acid sequestrants (BAS) (for primary BAD or ileal resection < 100 cm): c
- Cholestyramine or Colestipol (oral powders; may cause bloating, constipation, and poor compliance).
- Colesevelam (tablet formulation; better tolerated).
- Bile acid sequestrants (BAS) (for primary BAD or ileal resection < 100 cm): c
- Second-line:
- Dietary modification: Restricting fat intake to < 40 g/day to reduce bile acid stimulation of the colon.
- Extensive ileal resection (> 100 cm):
- Avoid BAS: Binding bile acids further depletes the already limited bile acid pool, worsening fat malabsorption and steatorrhea.
- Nutritional support: Low-fat diet supplemented with medium-chain triglycerides (MCTs) (absorbed directly without needing bile acid micelle formation).
- Parenteral Vitamin B12 and oral fat-soluble vitamins (A, D, E, K).
- First-line:
Treatment
Antidiarrheal agents
- Bismuth subsalicylate
- Converts to bismuth and salicylic acid in the GI tract
- Has antisecretory, antimicrobial, and antiinflammatory effects
- Can be used in bacterial diarrhea
- Loperamide
- Opioid receptor agonist that increases intestinal transit time
- Loperamide acts on intestinal μ-receptors and inhibits intestinal peristalsis and intestinal fluid secretion, and increases sphincter tone.
- Best initial treatment for chemotherapy-induced diarrhea
- Cautions
- Should not be used for > 48 hours without reevaluation of the patient
- Opioid receptor agonist that increases intestinal transit time
Warning
Loperamide should be avoided in patients with suspected invasive diarrhea with inflammatory features, as it reduces intestinal motility, which consequently increases the risk of bacterial colonization and invasion.