Epidemiology
Etiology
- Chronic heavy alcohol use (most common, esp. men)
- Pancreatic ductal obstruction
- Tobacco use
- Idiopathic pancreatitis
- Hereditary pancreatitis
- PRSS1 gene mutation
- Age of onset < 20 years
- Characterized by a positive family history and the absence of other risk factors
- Systemic disease
- Cystic fibrosis
- Severe hypertriglyceridemia (levels > 1,000 mg/dL)
Pathophysiology
Clinical features
- Epigastric abdominal pain (main symptom)
- Pain radiates to the back, is relieved on bending forward, and is exacerbated after eating. c
- Often associated with nausea and vomiting
- Features of pancreatic insufficiency: late manifestation (after 90% of the pancreatic parenchyma is destroyed)
- Steatorrhea (exocrine enzyme deficiency)
- Malabsorption and weight loss
- Pancreatic diabetes (endocrine hormone deficiency)
Complications
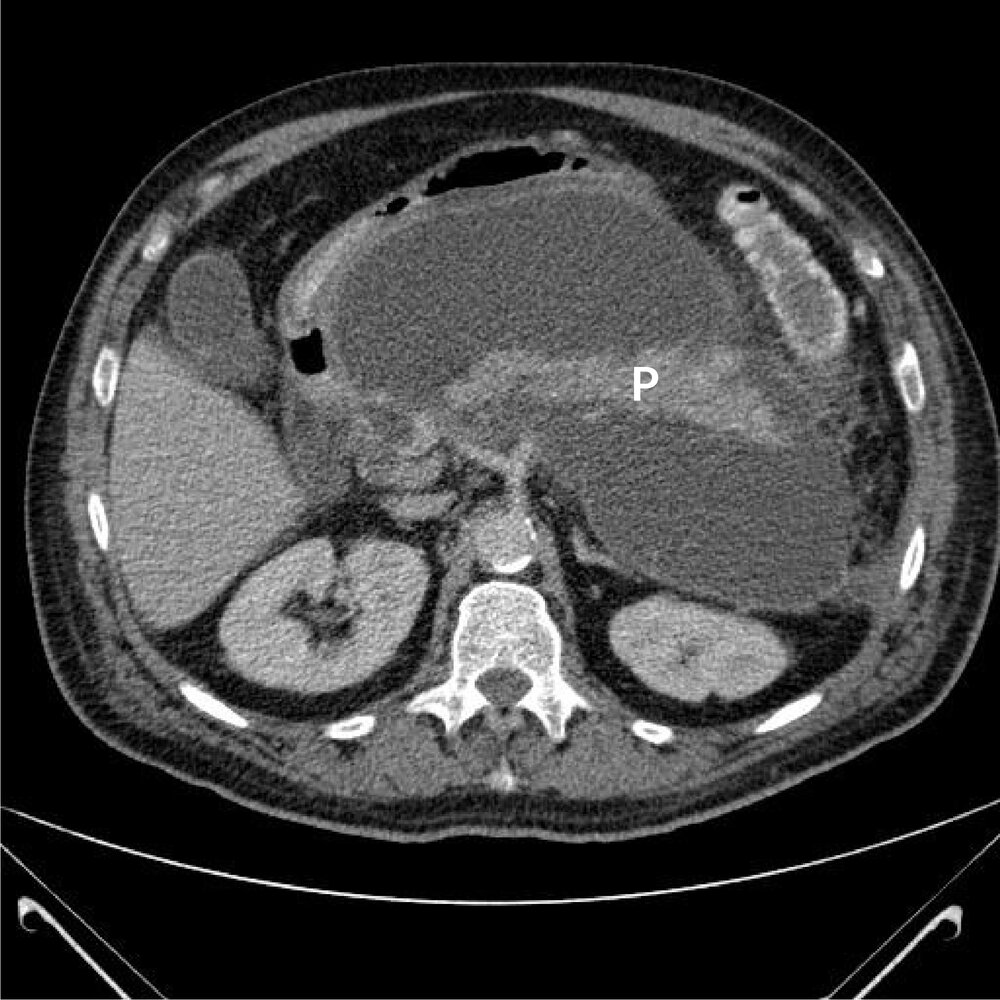
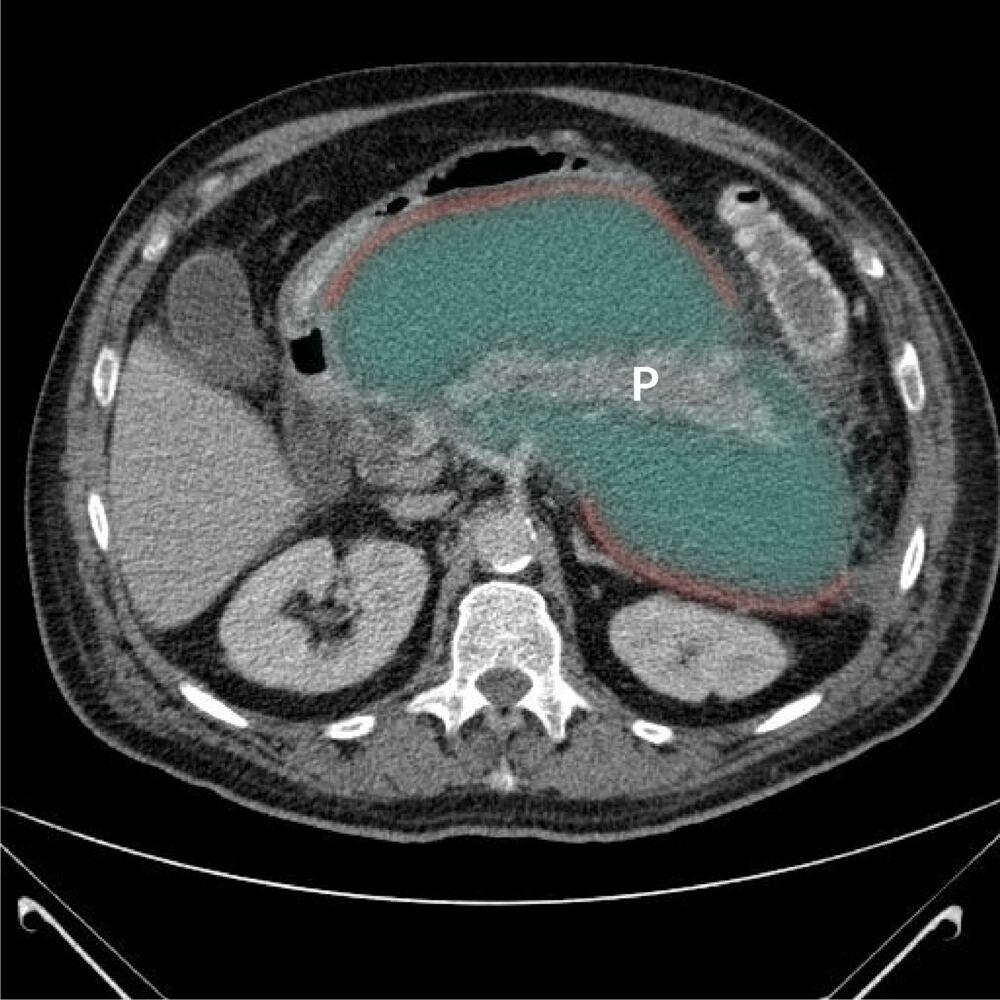
Pancreatic pseudocysts
- Pathology
- Fluid collection rich in enzymes (Amylase, Lipase) and necrotic debris.
- Lined by granulation tissue/fibrosis (NOT epithelium) “Pseudo” cyst. t
- Most common cystic lesion of pancreas.
- Etiology
- Acute Pancreatitis (complication appearing 4–6 weeks post-onset).
- Chronic Pancreatitis (most common).
- Trauma.
- Clinical Features
- Persistent epigastric pain/mass.
- Early satiety or N/V (mass effect on stomach/duodenum).
- Diagnostics
- CT Scan: Best initial test.
- Labs: Persistently Serum Amylase weeks after acute episode.
- Treatment
- Asymptomatic / < 6 cm: Conservative (Observation); spontaneous resolution common.
- Symptomatic / > 6 cm / > 6 weeks: Drainage required (Percutaneous, Endoscopic Cystogastrostomy, or Surgical).
Pancreatic ascites
Pathophysiology
- Ductal disruption (due to an acute attack of pancreatitis, pancreatic surgery and/or trauma) or a pseudocyst leak/rupture → pancreatic ascites
- Pancreatic ascites develops when the pancreatic leak is not walled off by fibrous/granulation tissue. It is a rare complication (∼ 1%) that is mostly seen in patients with chronic pancreatitis secondary to heavy alcohol use.
Diagnostics
Ascitic fluid analysis: exudate (high protein: inline-measurement; low SAAG: inline-measurement) with high amylase levels (> 1,000 IU/L)
Diagnostics
- Key Labs:
- Amylase & Lipase: Often normal or only mildly elevated in late-stage CP (burnt-out parenchyma). c
- Fecal elastase-1: Most sensitive and specific non-invasive functional test (<200 mcg/g indicates pancreatic insufficiency).
- 72-hour fecal fat collection: Diagnostic gold standard for steatorrhea but rarely used due to patient non-compliance.
- Imaging:
- Abdominal X-ray: High-yield if it shows pancreatic calcifications (highly specific for CP, but low sensitivity).
- Abdominal CT (Initial imaging of choice): Shows pancreatic calcifications, parenchymal atrophy, and pancreatic duct dilation. c
- MRCP (Confirmatory non-invasive test of choice): Exquisite visualization of ductal anatomy; reveals “chain of lakes” (alternating stenosis and dilation) or ductal stones.
- Endoscopic Ultrasound (EUS): Most sensitive test for early-stage CP when calcifications are not yet visible on CT/MRCP.
Treatment
- Exocrine Insufficiency (Malabsorption)
- Pancreatic Enzyme Replacement Therapy (PERT) containing lipase, amylase, and protease.
- Lipase is irreversibly inactivated at pH < 4.0. So use enteric-coated microspheres (delayed release) or PPI. t
- Indicated for steatorrhea and weight loss.
- Pancreatic Enzyme Replacement Therapy (PERT) containing lipase, amylase, and protease.