Primary lactase deficiency (lactase non-persistence): Most common cause. Genetically programmed down-regulation of lactase production after infancy. Common in Asian, African, and Native American populations.
The down-regulation happens because, for most of human history, it was no longer needed after infancy. The persistence of lactase is the exception, not the rule, for our species.
Secondary lactase deficiency: Due to damage to the small intestine mucosa (e.g., celiac disease, gastroenteritis, Crohn’s disease). Usually transient. c
Congenital lactase deficiency: Rare autosomal recessive disorder. Complete absence of lactase from birth.
Pathophysiology
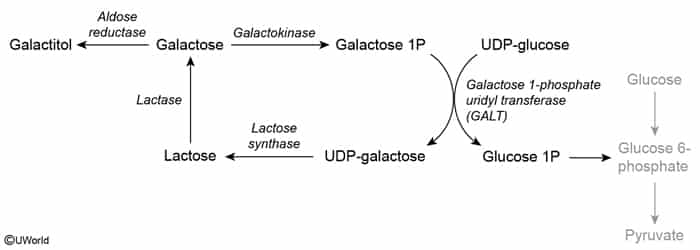
Lactase is a brush‑border enzyme that cleaves lactose, a disaccharide, into absorbable monosaccharides (galactose and glucose).
In the case of lactase deficiency, an almost complete absence of lactose digestion is observed, resulting in decreased absorption in the small intestine (particularly the jejunum).
The transfer of osmotically active amounts of lactose into the large intestine leads to the osmotic binding of water → diarrhea with a high osmotic gap
↓ Stool pH (< 6): due to lactose fermentation by colonic bacterial flora
Increased peristalsis due to increased intestinal filling → abdominal pain
Metabolism of lactose via the physiological bacterial flora of the colon
Formation of short‑chain fatty acids that exacerbate diarrhea
Increased gas formation and flatulence
Clinical features
Osmotic diarrhea, bloating, flatulence, and crampy abdominal pain occurring 30 mins to 2 hours post-dairy ingestion.
Lactose is widely used as an additive in non-dairy foods (e.g., processed meats, bread, baked goods, salad dressings) and as a filler in medications. A patient with lactase deficiency will experience symptoms after many standard mealsc
Borborygmi (hyperactive bowel sounds) and mild abdominal distension on physical exam.
Absence of systemic symptoms (no weight loss, fever, or hematochezia).
Diagnostics
Hydrogen breath test
The amount of hydrogen in the expired air increases after administering lactose in the fasting state.