Etiology
- Idiopathic
- Infectious
- Most commonly viral (e.g., coxsackie B virus)
- Bacterial (e.g., Staphylococcus spp., Streptococcus spp.)
- TB: Rare in the US/developed nations, but the most common cause of pericarditis in developing nations and endemic areas. c
- Myocardial infarction
- Postinfarction fibrinous pericarditis: within 1–3 days as an immediate reaction
- Dressler syndrome: weeks to months after an acute myocardial infarction
- Postoperative (postpericardiotomy syndrome): due to blunt or sharp trauma to the pericardium
- Uremia: e.g., due to acute or chronic renal failure
- Accumulated toxins promote inflammation.
- Radiation
- Exudative pericarditis: develops acutely during or after radiation therapy
- Constrictive pericarditis: develops several years after radiation therapy
- Neoplasms (e.g., Hodgkin lymphoma)
- Autoimmune connective tissue diseases (e.g., rheumatoid arthritis, SLE, scleroderma)
- Trauma
Classifications
- Serous Pericarditis
- Viral infection (Coxsackievirus, echovirus, adenovirus)
- Uremia
- TB pericarditis (early stage)
- Rheumatic fever
- Malignancy involvement
- SLE, Rheumatoid arthritis
- Fibrous or Fibrinous Pericarditis
- Most common pericarditis
- MI (Dressler syndrome)
- Rheumatic fever
- Uremia
- TB pericarditis
- Malignancy involvement
- Pericardial surface covered by shaggy, fibrinous exudate
- “Bread and Butter” appearance
- Purulent (Suppurative) Pericarditis
- Pyogenic bacteria (Staphylococci, Streptococci, Pneumococci)
- Direct extension / hematogenous or lymphatic spread / direct implant
- Severe acute infection
- Pericardial surface covered by purulent exudate and infiltrated by neutrophils
- Hemorrhagic Pericarditis
- Malignancy involvement
- TB pericarditis
- Severe acute infection
- Admixture of inflammatory effusion with blood
Clinical features
Acute pericarditis
- Chest Pain (CP): Pleuritic, sharp, retrosternal.
- Positional: Worse when supine; relieved by leaning forward.
- Radiation: Trapezius ridges (pathognomonic; phrenic nerve irritation).
- Physical Exam (PE): Pericardial Friction Rub (high-pitched, scratching/velcro sound; heard best at LLSB with pt leaning forward during expiration).
Chronic pericarditis
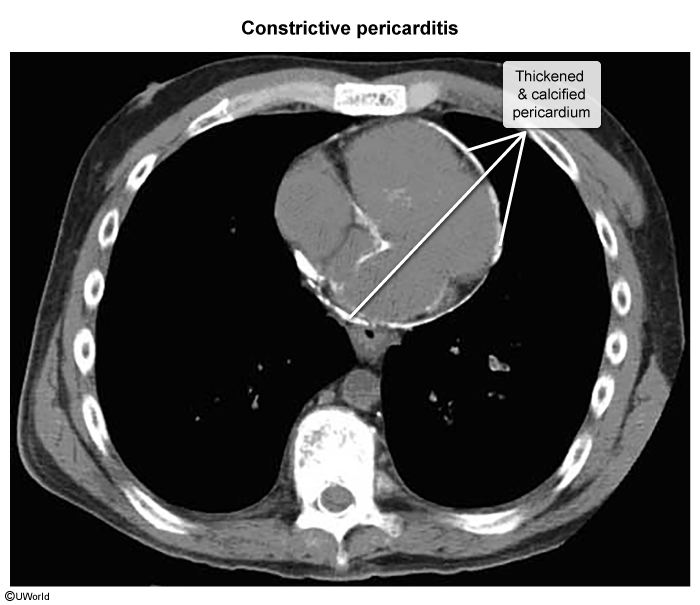
Constrictive pericarditis
- Pathophysiology: A late complication (sequela). Chronic fibrosis, scarring, and calcification of the pericardium leading to a rigid, non-compliant sac.
- Symptoms of fluid overload (i.e., backward failure)
- Jugular vein distention, ↑ jugular venous pressure
- Won’t seen in cirrhosis
- Jugular vein distention, ↑ jugular venous pressure
Hepatojugular Reflux (HJR) and Jugular vein distention (JVD)
- (+) HJR + ↑ JVP (Cardiac Etiology): Indicates elevated right-sided filling pressures. c
- Causes: Right heart failure (RHF), cor pulmonale, constrictive pericarditis, tricuspid valve disease, restrictive cardiomyopathy.
- (-) HJR + Normal JVP (Non-Cardiac Etiology): Indicates the RV can handle the increased preload.
- Causes: Primary liver disease (cirrhosis, portal HTN), Budd-Chiari syndrome, nephrotic syndrome, hypoalbuminemia.
- Kussmaul Sign: Paradoxical rise in JVD with inspiration (impaired RV filling). c
- Pericardial Knock: High-frequency early diastolic sound (caused by sudden cessation of ventricular filling). c
- Differ from S3, which is low-frequency early diastolic sound
Diagnostics
Acute pericarditis
- Clinical Dx: Requires ≥2 of 4: (1) Characteristic CP, (2) Friction rub, (3) EKG changes, (4) New/worsening pericardial effusion.
- Initial/Screening (EKG):
- Diffuse ST-elevation (concave/up-sloping) and PR-segment depression (highly specific). c
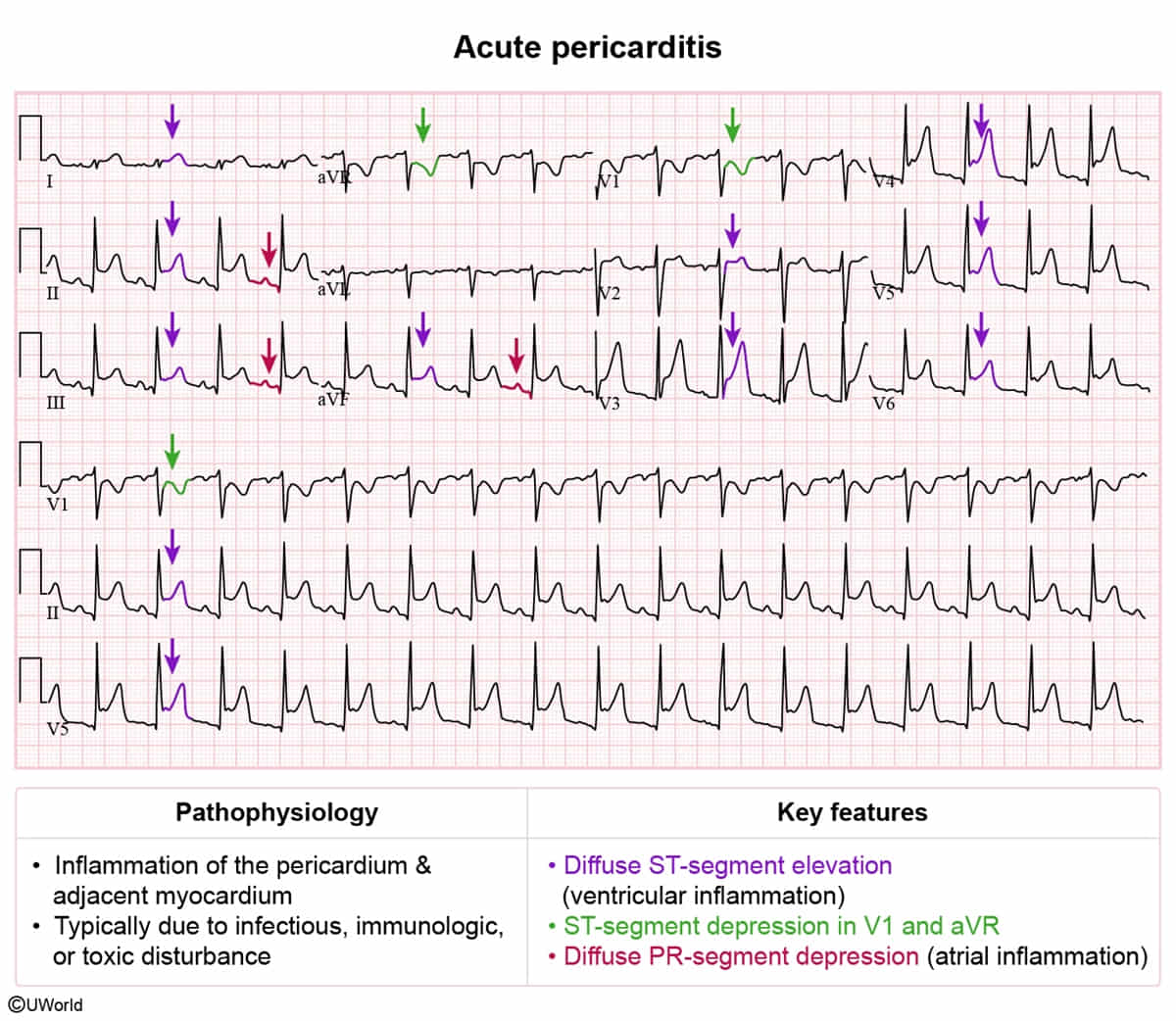
- Note: aVR will show ST-depression and PR-elevation.
- Diffuse ST-elevation (concave/up-sloping) and PR-segment depression (highly specific). c
- Key Labs: ↑ ESR, ↑ CRP, mild leukocytosis. ↑ Troponin I/T suggests perimyocarditis.
- Imaging:
- CXR: Usually normal. “Water-bottle heart” if large effusion (>200mL) present.
- Echocardiogram: Initial test to rule out effusion or tamponade; often normal in uncomplicated pericarditis.
Chronic pericarditis
- Imaging
- CT and cardiac MRI
- Pericardial thickening > 2 mm
- Calcifications
- CT and cardiac MRI
Treatment
- First-line (Idiopathic/Viral): NSAIDs (Ibuprofen or Indomethacin) + Colchicine (colchicine significantly ↓ recurrence rate). c
- Second-line / Refractory: Corticosteroids (Prednisone). Note: Avoid steroids as first-line unless NSAIDs are contraindicated (e.g., pregnancy, severe renal disease) or if etiology is autoimmune, due to high risk of recurrence.
- Etiology-Specific Variants:
- Post-MI: Aspirin + Colchicine (Avoid other NSAIDs & steroids; they impair myocardial scar formation and ↑ risk of ventricular free wall rupture).
- Uremic Pericarditis: Hemodialysis (NSAIDs/colchicine are ineffective and contraindicated).