Night sweats, weight loss > 10% in the past 6 months, fever > 38°C (100.4°F)
Pel-Ebstein fever: Intermittent fever with periods of high temperature for 1–2 weeks, followed by afebrile periods for 1–2 weeks. Relatively rare but very specific for HL.
Alcohol-induced pain: Pain in involved lymph nodes after ingestion of alcohol. Relatively rare but highly specific for HL.
Diagnostics
Histology
Lymph node excision
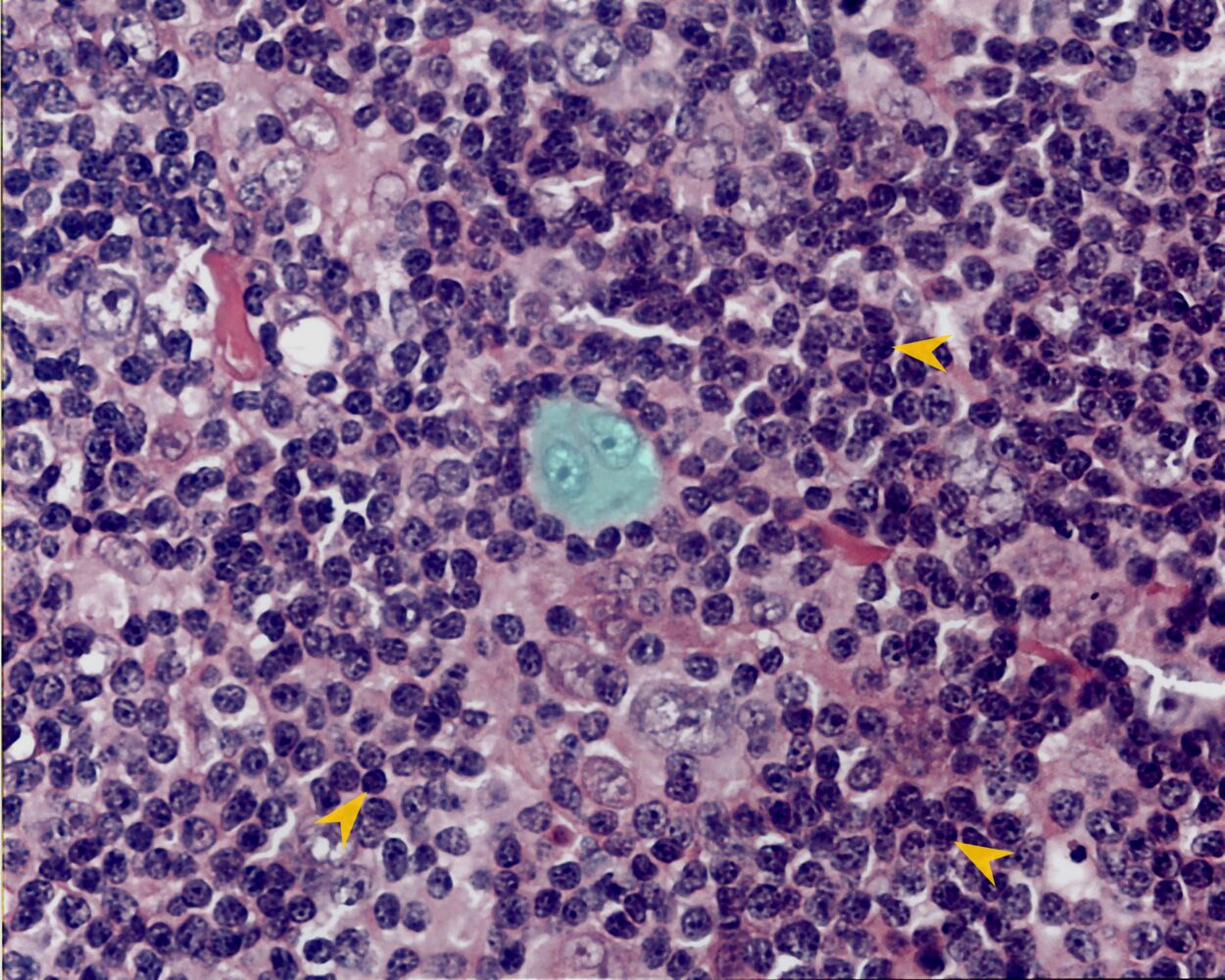
Reed-Sternberg cells (RSCs)
Tumor cells that are pathognomonic of HL
Originate from B cells
Large cells with binuclear/bilobed nuclei with dark centers of chromatin and pale halos, which results in an owl-eye appearance on histopathologic examination.
CD15/CD30-positive
Hodgkin cells: mononuclear, malignant B lymphocytes
Polynuclear RSCs are giant cells formed through the fusion of multiple Hodgkin cells.