Epidemiology
Etiology
- Primary (Essential) HTN: 90% of cases. Risk factors: Age, obesity, diabetes, smoking, genetics (2x risk if parents have HTN), African American ancestry, high Na+ intake, alcohol.
- Secondary HTN: 10% of cases. Suspect if resistant to 3+ meds or young patient (< 30 yo). c
- Renal: Renal Artery Stenosis (RAS). t
- Fibromuscular dysplasia: Young females (“string of beads” on angiogram).
- Atherosclerosis: Older males.
- Mechanism: ↓ renal perfusion → ↑ Renin → ↑ Angiotensin II/Aldosterone.
- Endocrine:
- Primary Hyperaldosteronism (Conn syndrome): HTN + Hypokalemia + ↓ Renin.
- Cushing syndrome: Weight gain, striae, buffalo hump.
- Pheochromocytoma: Episodic HA, sweating, tachycardia (5 P’s).
- Other: Obstructive Sleep Apnea (OSA), Coarctation of the Aorta (BP arms > legs, rib notching).
- Renal: Renal Artery Stenosis (RAS). t
Pathophysiology
Clinical features
Diagnostics
- Initial/Screening: Office BP. Diagnosis requires elevated BP (≥130/80 mmHg per ACC/AHA) on ≥2 separate occasions.
- Confirmatory/Gold Standard: Ambulatory BP monitoring (ABPM) or home BP monitoring (differentiates true HTN from White Coat HTN & Masked HTN).
- Key Labs/Imaging (Routine initial w/u for all new HTN): c2
- In order to identify complications of hypertension or comorbid conditions (eg, chronic kidney disease) that might influence management decisions.
- BMP (eval Cr for baseline renal function; K+ for hyperaldosteronism; fasting glucose/Ca2+).
- Fasting lipid panel.
- TSH.
- Urinalysis (screen for proteinuria/nephropathy).
- ECG (screen for LVH, prior silent MI).
Treatment
- Core Principles
- Goal: BP <130/80 mmHg for most patients.
- First-Line Agents: Thiazide diuretics, ACE inhibitors (ACEi)/ARBs, and Dihydropyridine CCBs.
- Foundation: Lifestyle modifications
- Weight Loss: Best overall if BMI > 25. Drops SBP 5-20 mm Hg per 10 kg lost.
- DASH Diet: Best if BMI is normal. High fruit/veg/low-fat dairy. Drops SBP 8-14 mm Hg.
- Exercise: ≥ 30 min/day aerobic. Drops SBP 4-9 mm Hg.
- Na+ Restriction: < 1.5–2 g/day. Drops SBP 2-8 mm Hg.
- EtOH Limitation: ≤ 2 drinks/day (men), ≤ 1 (women). Drops SBP 2-4 mm Hg.
- Calcium Kidney Stones
- Thiazide diuretic.
- Rationale: ↓ Urinary Ca concentration, preventing the supersaturation and precipitation of calcium-oxalate/phosphate stones.
- Thiazide diuretic.
- Special Populations
- African Americans: Thiazides or CCBs are preferred initial therapy.
- Pregnancy: Use Hydralazine, Methyldopa, Labetalol, Nifedipine (“He Makes Life Nice”).
- CI in Pregnancy: ACEi, ARBs, and renin inhibitors are teratogenic.
- High-Yield Adverse Effects
- ACEi: Dry cough, hyperkalemia, angioedema.
- Thiazides: Hypokalemia, hyperglycemia, hyperuricemia, hypercalcemia.
- Dihydro-CCBs: Peripheral edema, flushing, headache.
- β-blockers: Bradycardia, bronchoconstriction, sexual dysfunction.
- Spironolactone: Hyperkalemia, gynecomastia.
- Hypertensive Emergency
- Definition: SBP >180 or DBP >120 mmHg with acute end-organ damage.
- Tx: Use IV agents (e.g., labetalol, nicardipine). Lower Mean Arterial Pressure (MAP) by ≤25% in the first hour.
- Aortic Dissection Exception: Rapidly lower SBP to <120 mmHg with IV β-blockers (e.g., esmolol, labetalol).
Warning
In patients with long-standing hypertension, a chronic autoregulatory shift in the blood pressure–flow relationship occurs, affording less perfusion (flow) at any given pressure. Therefore, excessively rapid correction of blood pressure toward normal may induce relative ischemia.
Antihypertensive Selection by Comorbidity
- Coronary Atherosclerosis (CAD)
- Angina Pectoris: BB, CCB.
- Rationale: ↓ Myocardial O2 demand by ↓ HR and contractility.
- Post-MI: ACEi/ARB, BB.
- Rationale: BB ↓ risk of arrhythmias and sudden cardiac death; ACEi/ARB prevent adverse LV remodeling and ↓ mortality.
- Angina Pectoris: BB, CCB.
- Heart Failure with Reduced Ejection Fraction (HFrEF)
- ACEi/ARB, BB, MRA, Diuretics, DHP CCB.
- Rationale: ACEi, ARB, BB, and Aldosterone antagonists (MRA) provide proven mortality benefit and reverse remodeling. Diuretics manage volume (preload). DHP CCBs (e.g., Amlodipine) are safe for BP control if needed, unlike non-DHP CCBs.
- ACEi/ARB, BB, MRA, Diuretics, DHP CCB.
- Atrial Fibrillation (AFib) or Flutter
- BB, Non-DHP CCB (Diltiazem/Verapamil).
- Rationale: Provide rate control by slowing conduction through the AV node.
- BB, Non-DHP CCB (Diltiazem/Verapamil).
- Chronic Kidney Disease (CKD)
- ACEi or ARB.
- Rationale: Dilates the efferent arteriole, ↓ intraglomerular pressure and ↓ proteinuria; slows progression of renal failure.
- ACEi or ARB.
- Gout
- Losartan, other ARB, CCB (Avoid Thiazides/Loops). c
- Rationale: Losartan has uricosuric properties (↑ uric acid excretion). Diuretics compete with uric acid for secretion in the proximal tubule, triggering flares.
- Losartan, other ARB, CCB (Avoid Thiazides/Loops). c
- Osteoporosis
- Thiazide diuretic. c
- Rationale: ↓ Urinary Ca excretion by ↑ Ca reabsorption in the distal tubule; helps preserve bone mineral density.
- Thiazide diuretic. c
- Migraine
- BB, CCB.
- Rationale: First-line options for migraine prophylaxis via vascular stabilization and neuronal modulation.
- BB, CCB.
- Calcium Kidney Stones
- Thiazide diuretic.
- Rationale: ↓ Urinary Ca concentration, preventing the supersaturation and precipitation of calcium-oxalate/phosphate stones.
- Thiazide diuretic.
Complications
Eyes
- Hypertensive retinopathy
- Arteriosclerotic and hypertension-related changes of the retinal vessels
- Initial reactive vasoconstriction (vasospasm), followed by sclerosis with breakdown of blood-retinal barrier and subsequent hemorrhage and exudation
- Fundoscopic examination
- Cotton wool spots
- Retinal hemorrhages (i.e., flame-shaped hemorrhages)
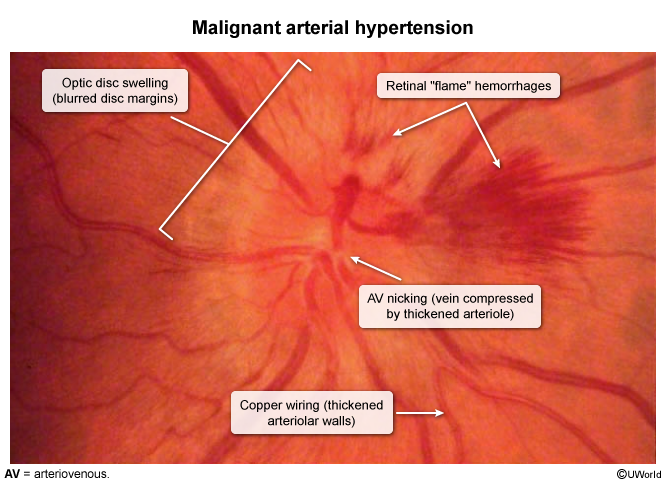
- Microaneurysms
- Macular star (results from exudation into the macula)
- Hard exudates
- Arteriovenous nicking: a tapering of a retinal venule at the point where a retinal arteriole crosses the retinal venule
- Marked swelling and prominence of the optic disk with indistinct borders due to papilledema and optic atrophy (end-stage disease)
- The presence of papilledema in a hypertensive patient may indicate a hypertensive crisis and warrants urgent lowering of blood pressure