Epidemiology
Etiology
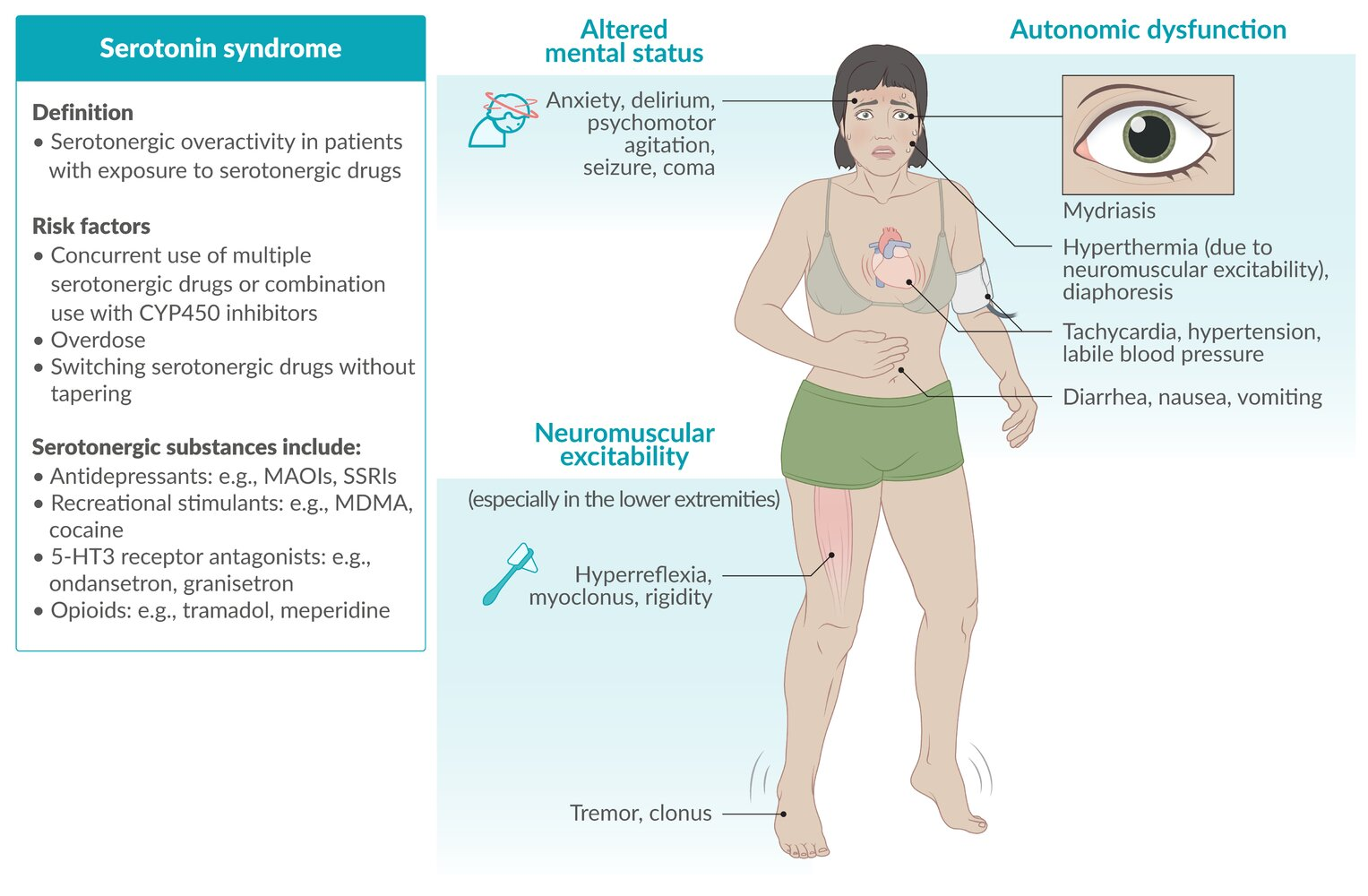
Serotonergic drugs
- Antidepressants (e.g., MAOIs, SSRIs, SNRIs, tricyclic antidepressants, vortioxetine, vilazodone, trazodone)
- Anxiolytics (e.g., buspirone)
- Anticonvulsants (e.g., valproate)
- Opioids (e.g., tramadol, meperidine)
- NMDA receptor antagonists (e.g., dextromethorphan)
- 5-HT3 receptor antagonists (e.g., ondansetron)
- Serotonin receptor agonists (e.g., triptans, ritonavir)
- Antibiotics (e.g., linezolid) t
- It possesses weak monoamine oxidase inhibitor (MAOI) activity. Co-administration of an MAOI (Linezolid) with a serotonergic agent (Paroxetine) prevents the breakdown of serotonin, leading to synaptic accumulation and toxicity.
- Herbal supplements (e.g., St. John’s wort, ginseng, tryptophan)
- Tryptophan is precursor of serotonin
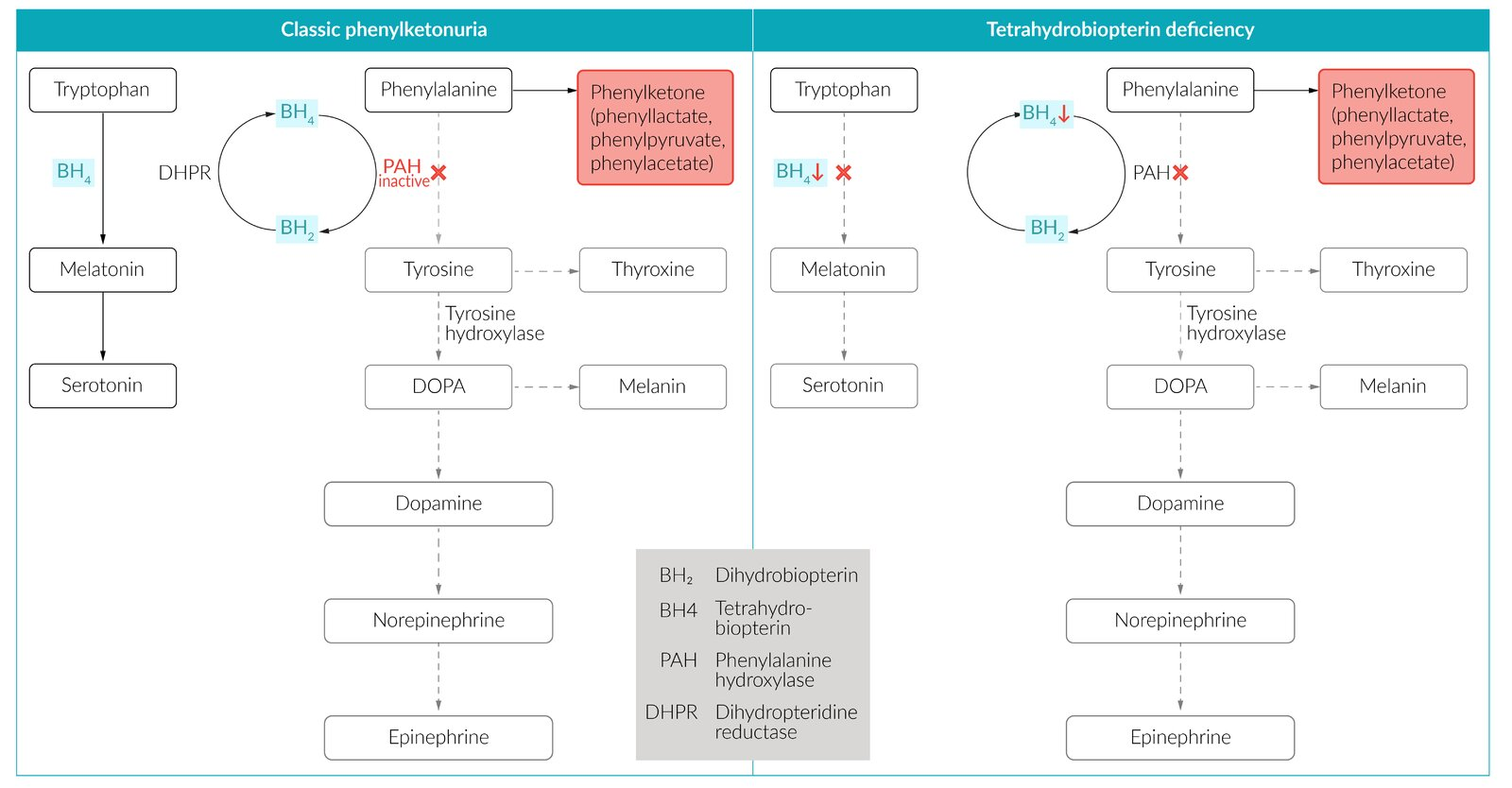
- Tryptophan is precursor of serotonin
- Recreational stimulants (e.g., MDMA, cocaine)
Tip
Serotonin syndrome rarely occurs with a single serotonergic drug used at therapeutic doses. More commonly, it is due to the combined effects of several serotonergic medications, overdose, and/or a drug-drug interaction. E.g. a depressed patient also takes linezolid.
Pathophysiology
Clinical features
- Rapid onset (usually within 24 hours of starting/increasing dose).
- Classic Triad:
- Mental Status Changes: Anxiety, agitation, delirium, confusion, coma.
- Autonomic Instability: Hyperthermia, tachycardia, hypertension, diaphoresis, diarrhea, mydriasis.
- Neuromuscular Hyperactivity: Hyperreflexia (lower extremities > upper), myoclonus, ocular clonus, tremor.
- Key distinction: Patients are reflexive and wet (diaphoretic), unlike anticholinergic toxicity (dry) or NMS (rigid).
Tip
- Patient is HOT and CRAZY + DRY = Anticholinergic
- Patient is HOT and CRAZY + WET & TWITCHY (Clonus) = Serotonin Syndrome
- Patient is HOT and CRAZY + STIFF (Rigidity) & HIGH CK = NMS
Tip
Sympathetic overactivity (dominant features) + GI hypermotility (the “exception”)
Diagnostics
Treatment
- Stop serotonergic agents immediately.
- Supportive: IV fluids + Benzodiazepines (1st line for agitation/tremor).
- Antidote: Cyproheptadine (5-HT2 antagonist) if unresponsive to benzos. t
- Hyperthermia: Active cooling; avoid antipyretics. Paralysis/intubation if severe.