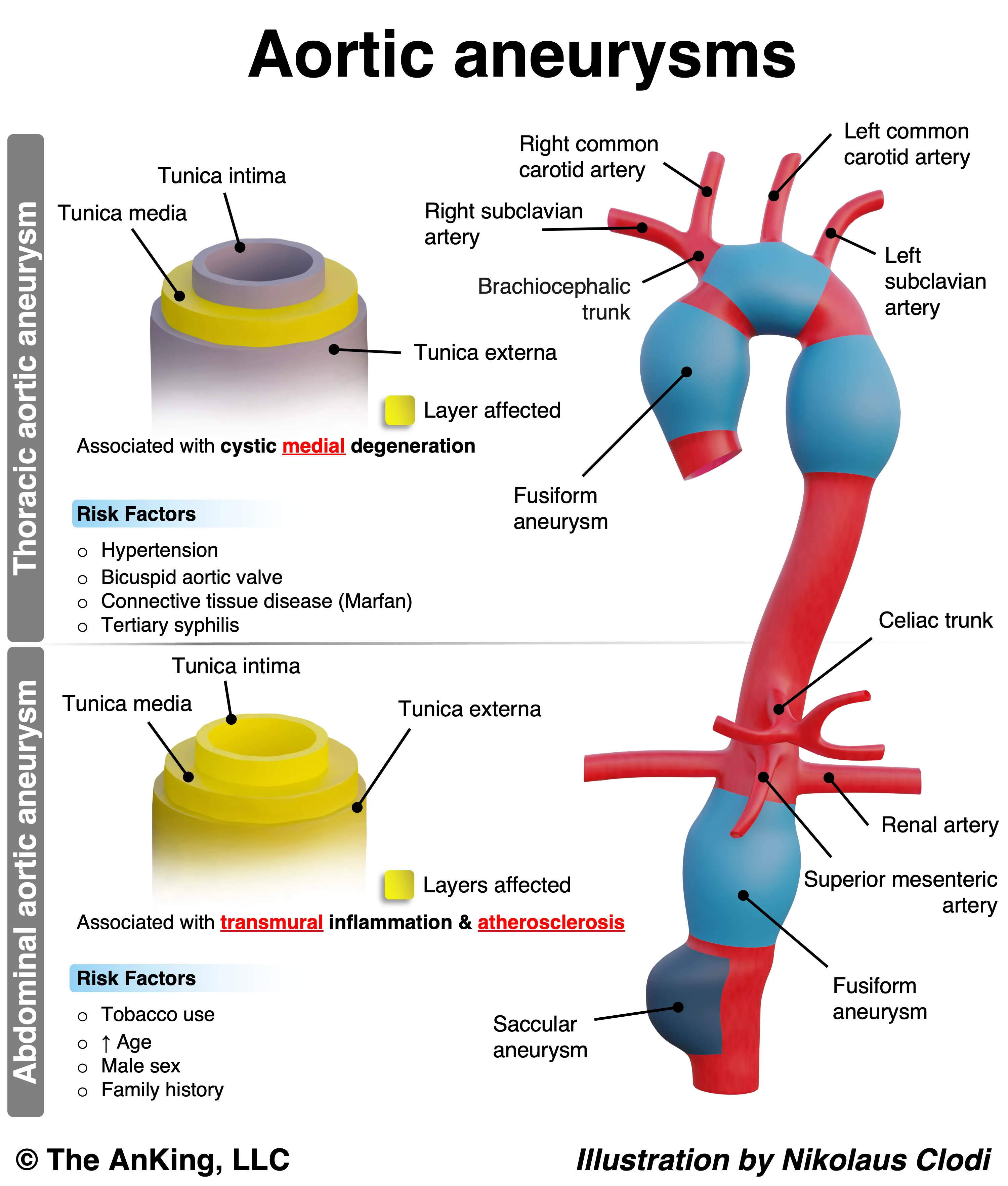
Abdominal Aortic Aneurysm (AAA)
- Etiology/Pathophysiology
- Most common true arterial aneurysm.
- Primary cause: Atherosclerotic cardiovascular disease, leading to chronic inflammation, elastin degradation, and weakening of the aortic wall.
- Location: Almost always infrarenal (below the renal arteries), partly due to the absence of vasa vasorum in this segment, making it more susceptible to ischemia.
- Defined as aortic diameter > 3.0 cm.
- Risk Factors
- Smoking: Strongest modifiable risk factor. c
- Age > 60-65 years.
- Male gender (4:1 ratio).
- Family history.
- Hypertension.
- Clinical Features
- Usually asymptomatic and found incidentally.
- Symptomatic:
- Pulsatile abdominal mass (buzzword).
- Dull abdominal or back pain.
- Rupture Triad (Surgical Emergency):
- Classic Triad: Severe acute abdominal/back pain + Pulsatile mass + Hypotension.
- Grey Turner sign (flank ecchymosis) or Cullen sign (periumbilical ecchymosis) = retroperitoneal bleed.
- Diagnostics
- Screening (USPSTF): One-time Abdominal Ultrasound (US) in Men 65–75 who have ever smoked. c
- Symptomatic & Hemodynamically Stable: CT Angiography (CTA) of Abd/Pelvis (Gold standard for pre-op planning).
- Symptomatic & Hemodynamically Unstable: Bedside Focused Assessment with Sonography for Trauma (FAST) US.
- If (+) for AAA → Immediate OR (do not delay for CT).
- If (-) for AAA → Investigate other causes of shock.
- Incidental Finding: If found on X-ray/Palpation → Confirm w/ US.
- X-ray showing prevertebral calcifications, representing extensive atherosclerosis of the abdominal aorta c
- Treatment
- Conservative management for aneurysms < 5.5 cm:
- Smoking cessation.
- BP control (e.g., beta-blockers).
- Serial ultrasound monitoring.
- Surgical Repair: Indicated if:
- Diameter > 5.5 cm in men or > 5.0 cm in women.
- Rapid growth (>0.5 cm in 6 months or >1 cm per year).
- Presence of symptoms or rupture.
- Options: Open repair or Endovascular Aneurysm Repair (EVAR).
- Conservative management for aneurysms < 5.5 cm:
Thoracic Aortic Aneurysm (TAA)
- Etiology/Pathophysiology
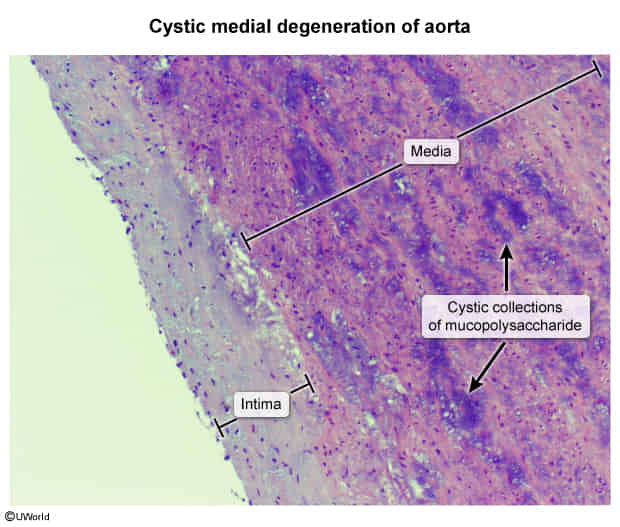
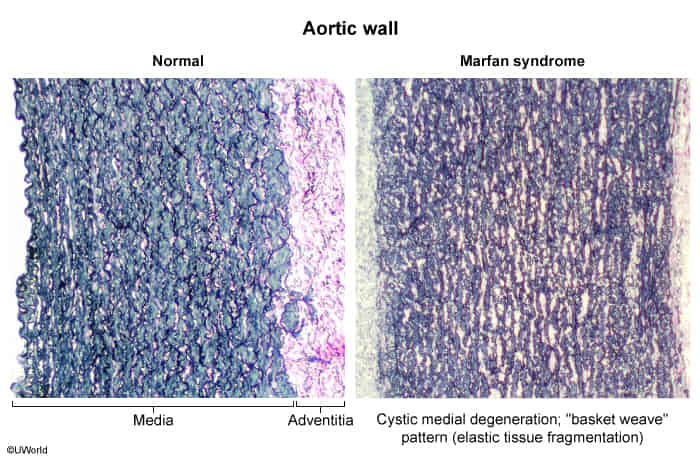
- Primary cause: Cystic medial necrosis, a degenerative process of the aortic media.
- It is characterized by the breakdown and loss of the structural components that give the aortic wall its strength and elasticity.
- This loss of structural elements leads to the formation of small, empty spaces or “cysts” that fill with a basophilic, mucopolysaccharide-rich substance (mucoid material).
- Associated Conditions:
- Connective tissue diseases: Marfan syndrome (FBN1 gene mutation) and Ehlers-Danlos syndrome (collagen defects).
- Bicuspid aortic valve.
- Tertiary syphilis (obliterative endarteritis of the vasa vasorum) → classic “tree-bark” appearance of the aorta.
- Location: Most commonly involves the ascending aorta.
- Primary cause: Cystic medial necrosis, a degenerative process of the aortic media.
- Risk Factors
- Hypertension.
- Connective tissue disorders (Marfan, Ehlers-Danlos).
- Family history.
- Smoking.
- Clinical Features
- Mostly asymptomatic.
- Symptomatic (due to compression of adjacent structures):
- Rupture/Dissection: Presents as sudden, severe, tearing chest pain radiating to the back.
- Diagnostics
- Initial/Incidental Finding: Often seen as a widened mediastinum on chest X-ray.
- Definitive Dx: CT angiography is the gold standard for diagnosis and pre-operative planning.
- Treatment
- Medical management:
- Strict BP control, with beta-blockers being first-line to reduce aortic wall shear stress.
- Activity restriction (e.g., avoiding heavy lifting).
- Surgical Repair: Indicated if:
- Diameter > 5.5-6.0 cm for ascending aorta.
- Diameter > 5.0 cm in patients with Marfan syndrome.
- Rapid growth.
- Presence of symptoms or dissection.
- Options: Open surgical repair or Thoracic Endovascular Aortic Repair (TEVAR).
- Medical management:
| Feature | Abdominal Aortic Aneurysm (AAA) | Thoracic Aortic Aneurysm (TAA) | Aortic Dissection |
|---|---|---|---|
| Patho | True aneurysm; Wall weakening | True aneurysm; Wall weakening | Intimal tear, false lumen |
| Location | Infrarenal | Ascending or Descending | Stanford A (Ascending), B (Descending) |
| #1 Risk Factor | Atherosclerotic cardiovascular disease (Smoking) | Hypertension / Marfan | Hypertension |
| Presentation | Usually asymptomatic, pulsatile mass | Usually asymptomatic, compression Sx | Tearing chest pain radiating to back |
| Key Finding | Pulsatile abdominal mass | Aortic regurgitation murmur | Asymmetric BPs or pulses |
| Dx | Ultrasound (screening) | CT Angiography (CTA) | CTA (stable), TEE (unstable) |
| Tx | Repair if >5.5 cm or symptomatic | Repair if >5.5 cm or symptomatic | A: Surgery B: Medical (β-blockers) |
Popliteal Artery Aneurysm
- Epidemiology & Risk Factors
- Most common peripheral aneurysm. Males >60. RFs: Atherosclerosis, smoking.
- HY Associations: 50% bilateral. 40-50% have concurrent AAA (must screen!).
- Clinical Features
- Asymptomatic: Bounding popliteal pulse / pulsatile mass.
- Symptomatic (Thromboembolism): Acute Limb Ischemia (ALI - 6 P’s). Note: Rupture is rare.
- Mass Effect: Compresses vein (mimics DVT) or tibial nerve.
- Diagnosis
- Initial/Confirmatory: Duplex U/S.
- Operative Planning: CTA or MRA.
- Required Secondary Screening: Abdominal U/S (to rule out concurrent AAA) and contralateral knee U/S (to rule out bilateral PAA). c
- Differential Diagnostics
- Baker Cyst: Non-pulsatile, transilluminates, posterior knee pain (assoc w/ OA/RA).
- DVT: Non-pulsatile, non-compressible popliteal vein on U/S.
- Popliteal Entrapment Syndrome: Young athletes; claudication triggered by plantar flexion.
- Management
- Asymptomatic < 2 cm: Observe, U/S surveillance, RF mod (statin, ASA).
- Asymptomatic > 2 cm OR +Thrombus: Elective repair (surgical bypass or endo stent).
- Symptomatic (ALI): Urgent catheter-directed thrombolysis OR open embolectomy + bypass.
- Complications
- ALI / Irreversible ischemia.
- Amputation.