Epidemiology
Etiology
Tip
- <60-65 years: Congenital bicuspid aortic valve is the most common cause. The altered hemodynamics across two leaflets instead of three leads to premature fibrosis and calcification.
- >65-70 years: Degenerative (senile) calcific stenosis of a previously normal tricuspid valve is the most common cause.
- Aortic valve sclerosis: calcification and fibrosis of aortic valve leaflets
- Most common cause of aortic stenosis
- Occurs at an increasing rate as patients age (prevalence is 35% in those aged 75–85 years)
- Similar pathophysiology to Atherosclerotic cardiovascular disease
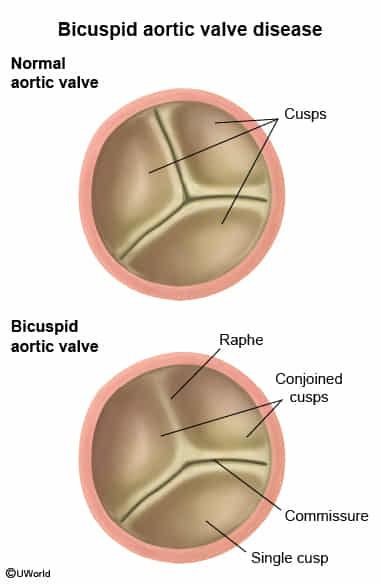
- Bicuspid aortic valve (BAV): fusion of two of the three aortic-valve leaflets in utero
- Most common congenital heart valve malformation, predominantly affects males (3:1)
- Predisposes the valve to dystrophic calcification and degeneration
- Bicuspid Aortic Valve can cause both Aortic Stenosis (AS) and Aortic Regurgitation (AR), though AS is the most common complication overall. c
- AR often presents earlier than AS (e.g., 20s or 30s) if due to prolapse, or acutely if secondary to IE.
Pathophysiology
Clinical features
- Symptoms (SAD Triad): Syncope (exertional), Angina, Dyspnea (HF).
- Prognosis post-symptom onset: HF (2 yrs) < Syncope (3 yrs) < Angina (5 yrs, severe phase). c
- Due to increased LV oxygen demand and reduced coronary flow reserve
- Signs and symptoms
- Physical Exam
- Pulses: Pulsus parvus et tardus (weak and delayed carotid upstroke) + narrow pulse pressure t
- Harsh crescendo-decrescendo (diamond-shaped), late systolic ejection murmur that radiates bilaterally to the carotids
- Best heard in the 2nd right intercostal space
- Handgrip decreases the intensity of the murmur.
- Valsalva and standing from squatting decreases or does not change the intensity of the murmur (in contrast to hypertrophic cardiomyopathy).
- “Late-peaking” murmur in severe AS, because as the valve becomes more stenotic, the Left Ventricle requires more time to build up sufficient pressure to overcome the obstruction and eject blood. t
- Soft, single S2
- A soft S2 results from a delay in the aortic component (A2) and softer closing of the aortic valve due to reduced mobility.
- S4 is best heard at the apex.
- Because of decreased compliance of the LV
- Early systolic ejection click
- Results from the abrupt stop of the valve leaflets upon opening
Diagnostics
- Initial/Screening: Transthoracic Echocardiogram (TTE).
- Determines severity. Severe AS: Valve area ≤ 1.0 cm², mean gradient ≥ 40 mm Hg, peak velocity ≥ 4 m/s. t
- Key Labs/Imaging:
- ECG: Shows LVH w/ strain pattern, LA enlargement.
- CXR: Aortic valve calcification, post-stenotic aortic dilation, LV prominence.
- BNP/pro-BNP: Elevated in decompensated HF.
- Confirmatory/Gold Standard: Cardiac catheterization (only if TTE is inconclusive or discrepancies exist b/w clinical exam and echo).
Treatment
- Asymptomatic (LVEF > 50%): Observation and serial TTEs (every 6-12 months for severe AS).
- Symptomatic OR Asymptomatic w/ LVEF < 50% OR undergoing other cardiac surgery: Aortic Valve Replacement (AVR).
- Surgical AVR (SAVR): Preferred in pts with low surgical risk. (Mechanical valve if < 50-65 yrs; Bioprosthetic if > 65 yrs).
- Transcatheter AVR (TAVR): Preferred in pts with high/prohibitive surgical risk or older age (> 80 yrs).
- Medical Management: AS pts are highly preload dependent. Use diuretics, nitrates, and vasodilators with extreme caution to avoid severe hypotension.