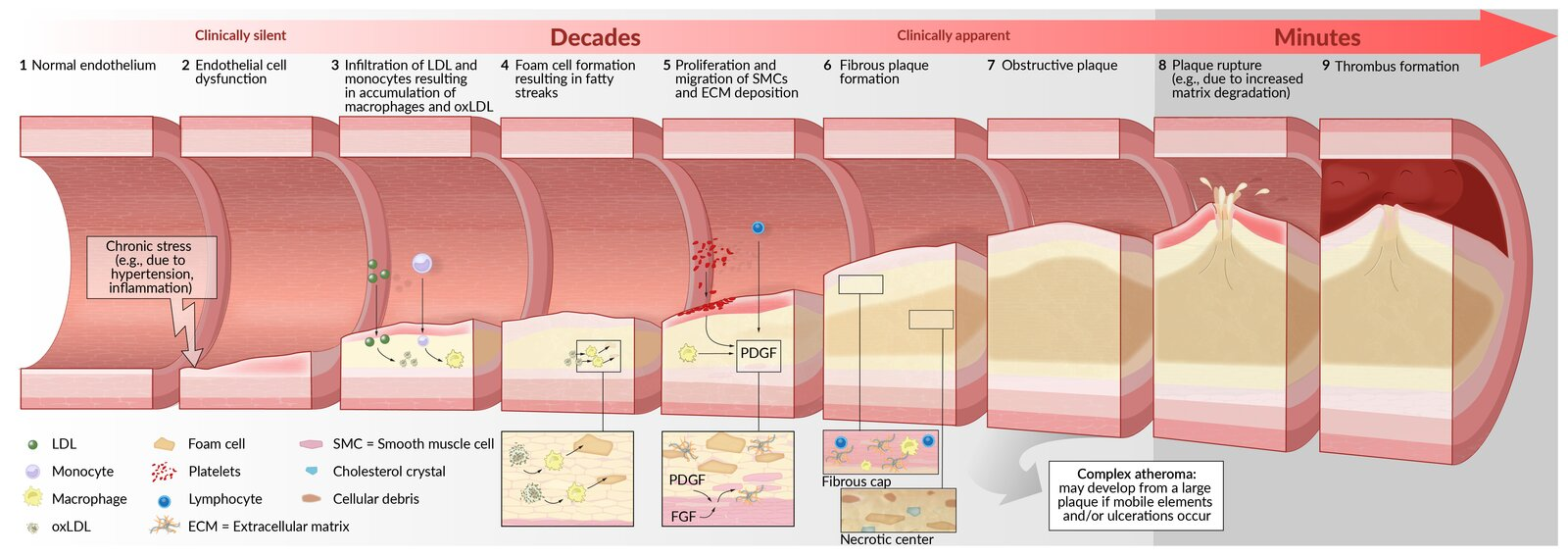
Chronic stress on the endothelium (e.g., due to arterial hypertension and turbulence)
Endothelial cell dysfunction, which leads to:
Invasion of inflammatory cells (mainly monocytes and lymphocytes) through the disrupted endothelial barrier
Adhesion of platelets to the damaged vessel wall → platelet release of inflammatory mediators (e.g., cytokines) and platelet-derived growth factor (PDGF)t
PDGF stimulates the migration and proliferation of smooth muscle cells (SMCs) in the tunica intima and mediates the differentiation of fibroblasts into myofibroblasts
Inflammation of the vessel wall
Macrophages and SMCs ingest cholesterol from oxidized LDL and transform into foam cells (macrophages filled with lipid droplets).
Foam cells accumulate to form fatty streaks (early atherosclerotic lesions).
Lipid-laden macrophages and SMCs produce extracellular matrix (e.g., collagen) deposition → development of a fibrous plaque (atheroma)
Macrophages, smooth muscle cells, lymphocytes, and extracellular matrix form a fibrous cap, which covers a necrotic center, consisting of foam cells, free cholesterol crystals, and cellular debris.
Inflammatory cells in the atheroma (e.g., macrophages) secrete matrix metalloproteinases → weakening of the fibrous cap of the plaque due to the breakdown of extracellular matrix → minor stress ruptures the fibrous cap
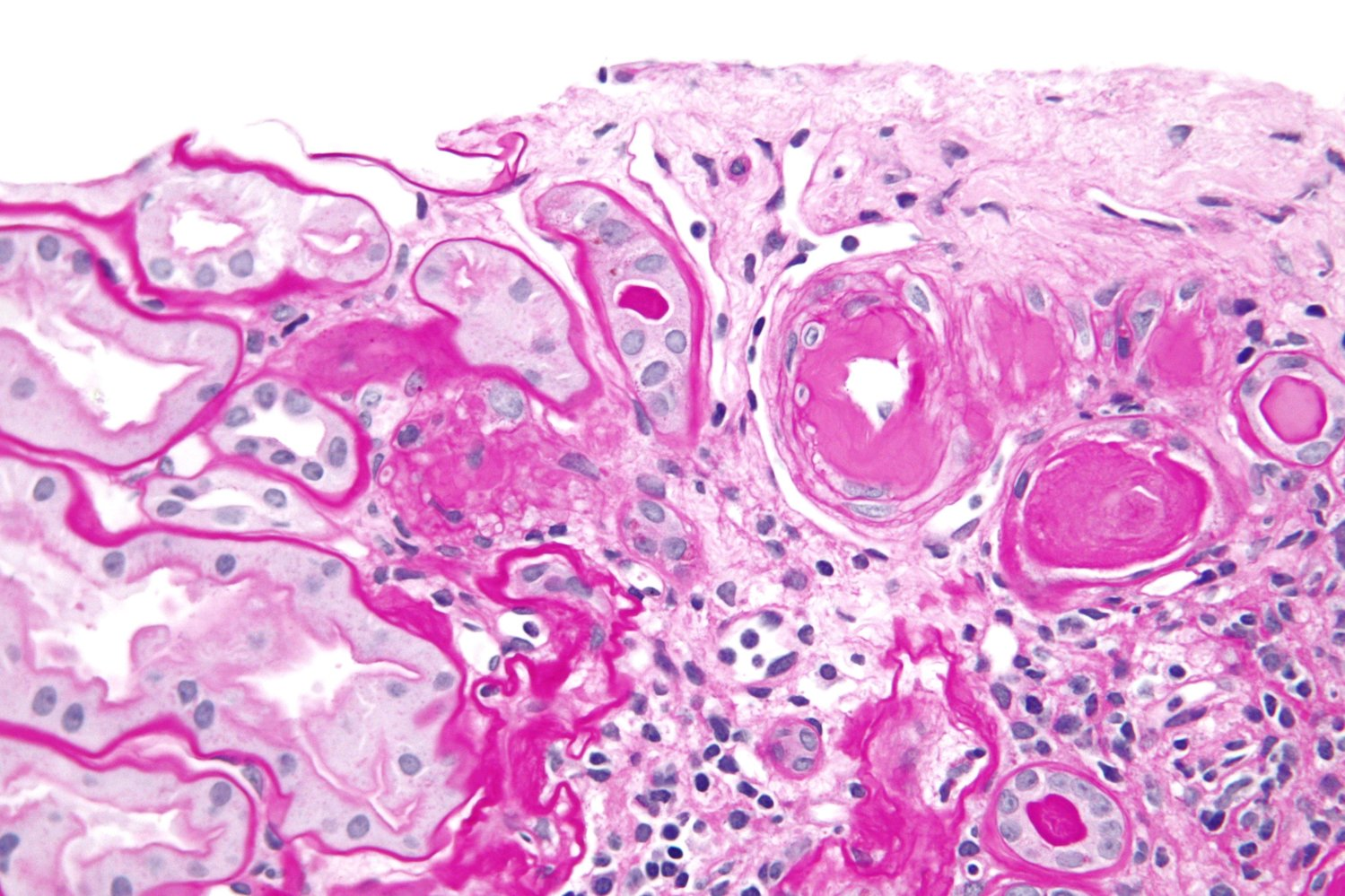
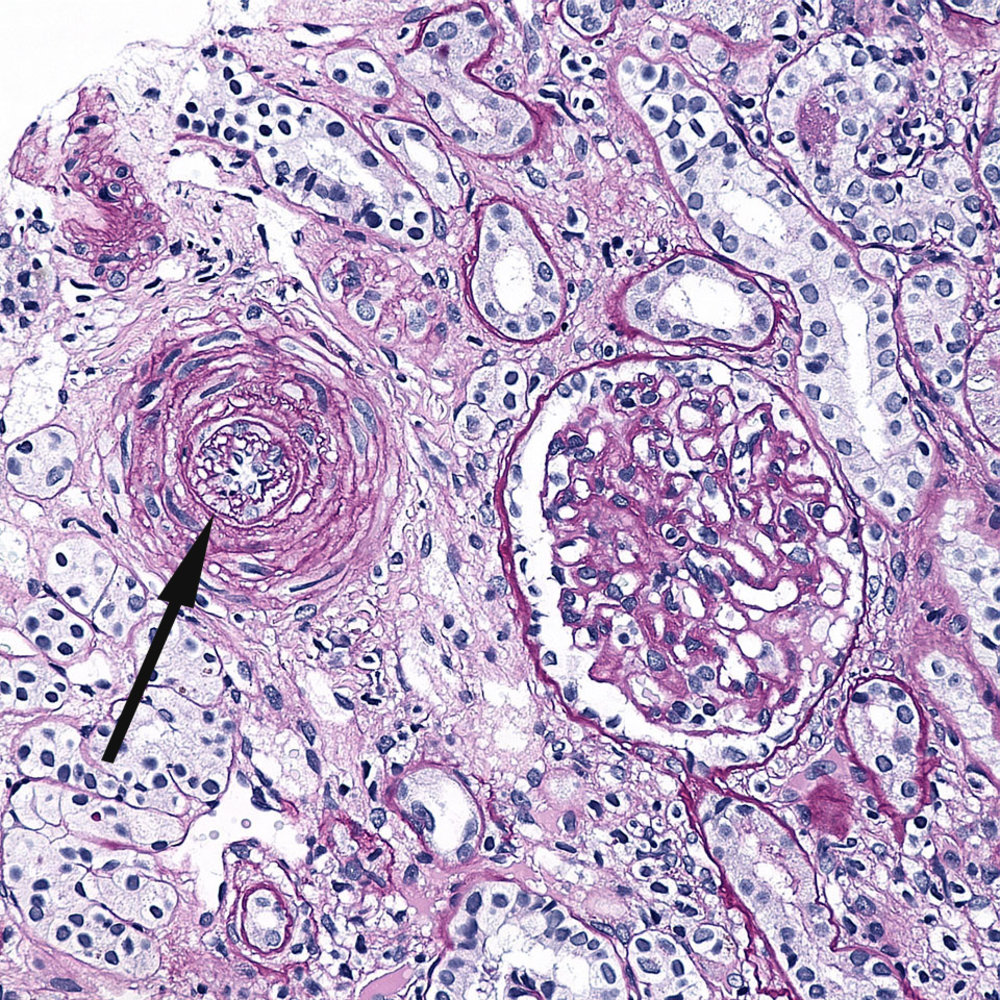
Calcification of the intima (the amount and pattern of calcification affect the risk of complications)
Plaque rupture → exposure of thrombogenic material (e.g., collagen) → thrombus formation with vascular occlusion or spreading of thrombogenic material
Aspirin: Routine primary prevention no longer recommended for adults >60 due to bleeding risk. Consider only in select high-risk adults 40-59 w/ low bleeding risk.