Epidemiology
Etiology
- Most commonly due to the following conditions:
- Bilateral idiopathic hyperplasia of the adrenal glands (∼ 60%)
- Aldosterone-producing adrenal adenoma or aldosteronoma (∼ 30%)
Pathophysiology
Autonomous aldosterone secretion and hypertension
- Physiological aldosterone secretion is regulated by the renin-angiotensin-aldosterone system (RAAS) and occurs in response to the detection of low blood pressure in the kidneys.
- ↑ Aldosterone → ↑ open Na+ channels in principal cells of luminal membrane at the cortical collecting ducts of the kidneys → ↑ Na+ reabsorption and retention → water retention → hypertension
- Aldosterone escape
- Definition: Evasion of the Na+-retaining effects of inappropriately elevated aldosterone levels in primary hyperaldosteronism
- Mechanism: sodium and water retention → volume expansion → secretion of atrial natriuretic peptide (ANP) and pressure natriuresis → compensatory diuresis → “escape” from edema formation and hypernatremia
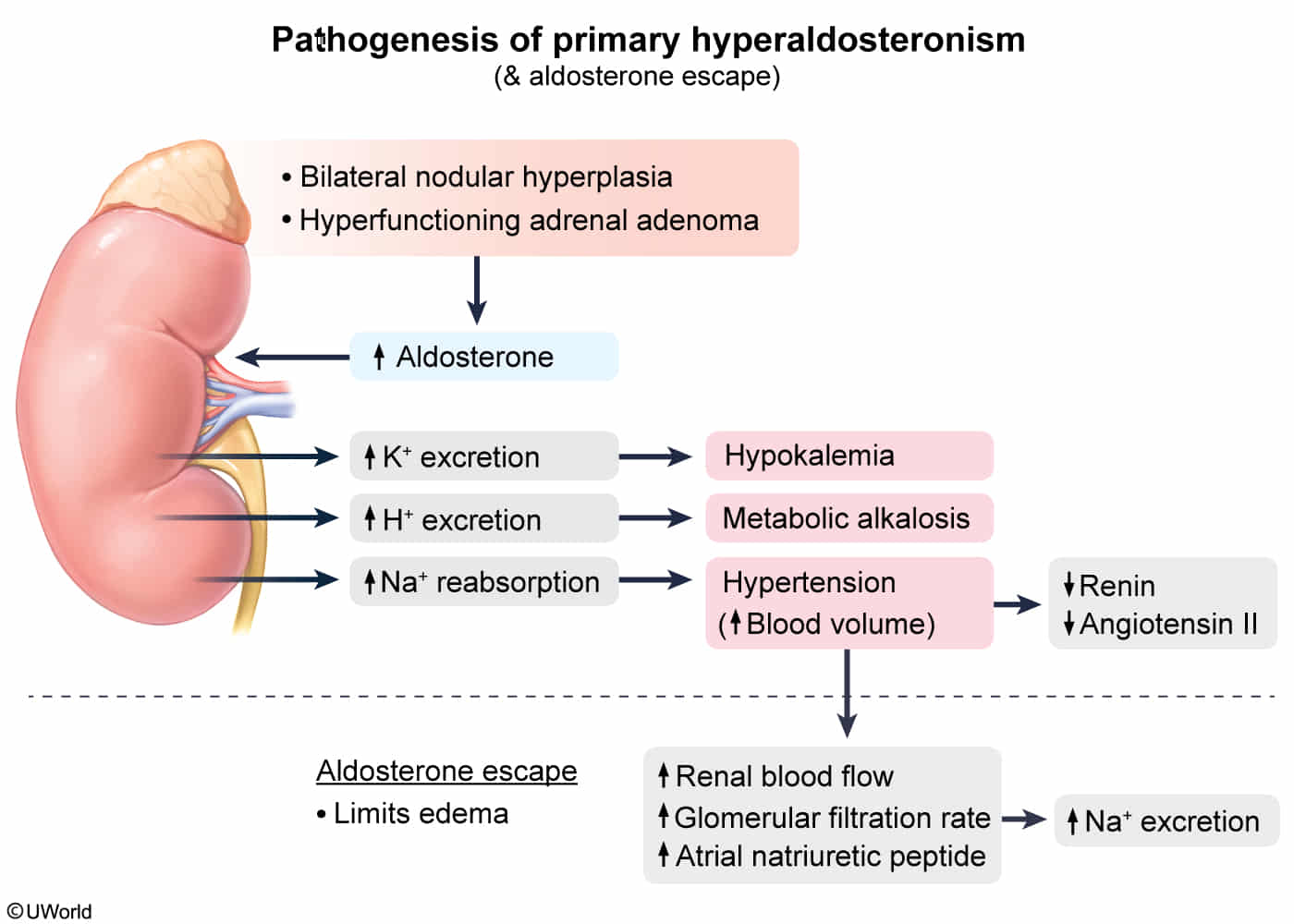
Hypokalemia and metabolic alkalosis
- ↑ Na+ reabsorption → electronegative lumen → electrical gradient through open K+ channels → ↑ K+ secretion → hypokalemia
- Hypokalemia → metabolic alkalosis via two mechanisms (both of which decrease extracellular H+, thereby increasing extracellular pH):
- Efflux of K+ from intracellular to extracellular space in exchange for H+
- ↑ H+ secretion in the kidney in order to enable ↑ K+ reabsorption
- Diabetes insipidus: hypokalemia → desensitization of renal tubules to antidiuretic hormone (ADH) → polyuria and polydipsia
Clinical features
- Hypertension
- Features of hypokalemia
- Fatigue
- Muscle weakness, cramping
- Headaches
- Absence of significant edema (due to aldosterone escape)
Tip
Primary hyperaldosteronism is characterized by hypokalemia and drug-resistant hypertension.
Diagnostics
- Initial/Screening: Morning Plasma Aldosterone Concentration (PAC) to Plasma Renin Activity (PRA) ratio.
- (+) Screen = PAC/PRA ratio > 20 w/ PAC > 15 ng/dL (High Aldo, Low Renin). c
- Must hold mineralocorticoid receptor antagonists (spironolactone/eplerenone) for up to 4-6 weeks prior.
- Confirmatory: Salt-loading test (Oral NaCl or IV Saline infusion).
- Normal response: High Na load suppresses aldosterone.
- Primary hyperaldosteronism: Failure to suppress aldosterone.
- Imaging: Adrenal CT to look for adenoma vs. bilateral hyperplasia.
- Gold Standard/Surgical Planning: Adrenal Venous Sampling (AVS).
- Essential to differentiate unilateral adenoma vs. bilateral hyperplasia if CT is equivocal, or in pts > 40yo (due to high prevalence of non-functioning incidentalomas).
Differential diagnostics
Secondary hyperaldosteronism
- Etiology
- Renal artery stenosis (e.g., due to Atherosclerotic cardiovascular disease, fibromuscular dysplasia)
- Renin-secreting tumor
- Chronic kidney disease
- Advanced CHF
- Fibromuscular dysplasia
- Liver cirrhosis
- Diuretics
- Laxative abuse
- Diagnostics: ↑ PAC (Plasma aldosterone concentration) and ↑ PRA (Plasma renin activity)
Treatment
- Unilateral disease or adrenal carcinoma: surgery preferred
- Bilateral disease: medical management preferred
- Bilateral adrenalectomy has a low success rate for curing hypertension and also leaves the patient dependent on lifelong glucocorticoid replacement; for this reason, medical management is recommended for bilateral disease.
Medical management
- First-line: aldosterone receptor antagonists
- Spironolactone (preferred)
- Eplerenone
- In contrast to spironolactone, eplerenone does not block androgen or progesterone receptors, which decreases certain side effects (e.g., gynecomastia and decreased libido); however, eplerenone is only half as potent at blocking the mineralocorticoid receptor and is less effective at lowering blood pressure.