Cholesterol embolization syndrome is a condition in which cholesterol crystals dislodge from atherosclerotic plaques and enter the bloodstream, blocking small to medium arteries in various organs.
Epidemiology
Etiology
- Pts w/ severe, diffuse atherosclerosis (HTN, hyperlipidemia, smoking).
- Typically occurs days to weeks following a vascular procedure (e.g., PCI, angiography, aortic surgery). c
- Can be triggered by initiation of anticoagulation or thrombolytics (destabilizes plaques).
- Rarely spontaneous.
Pathophysiology
Atherosclerosis → rupture of atherosclerotic plaque (most commonly from the aorta) → blockage and inflammation of small to medium arteries by cholesterol crystals → formation of multiple small peripheral, muscular, or visceral emboli → end-organ damage
Clinical features
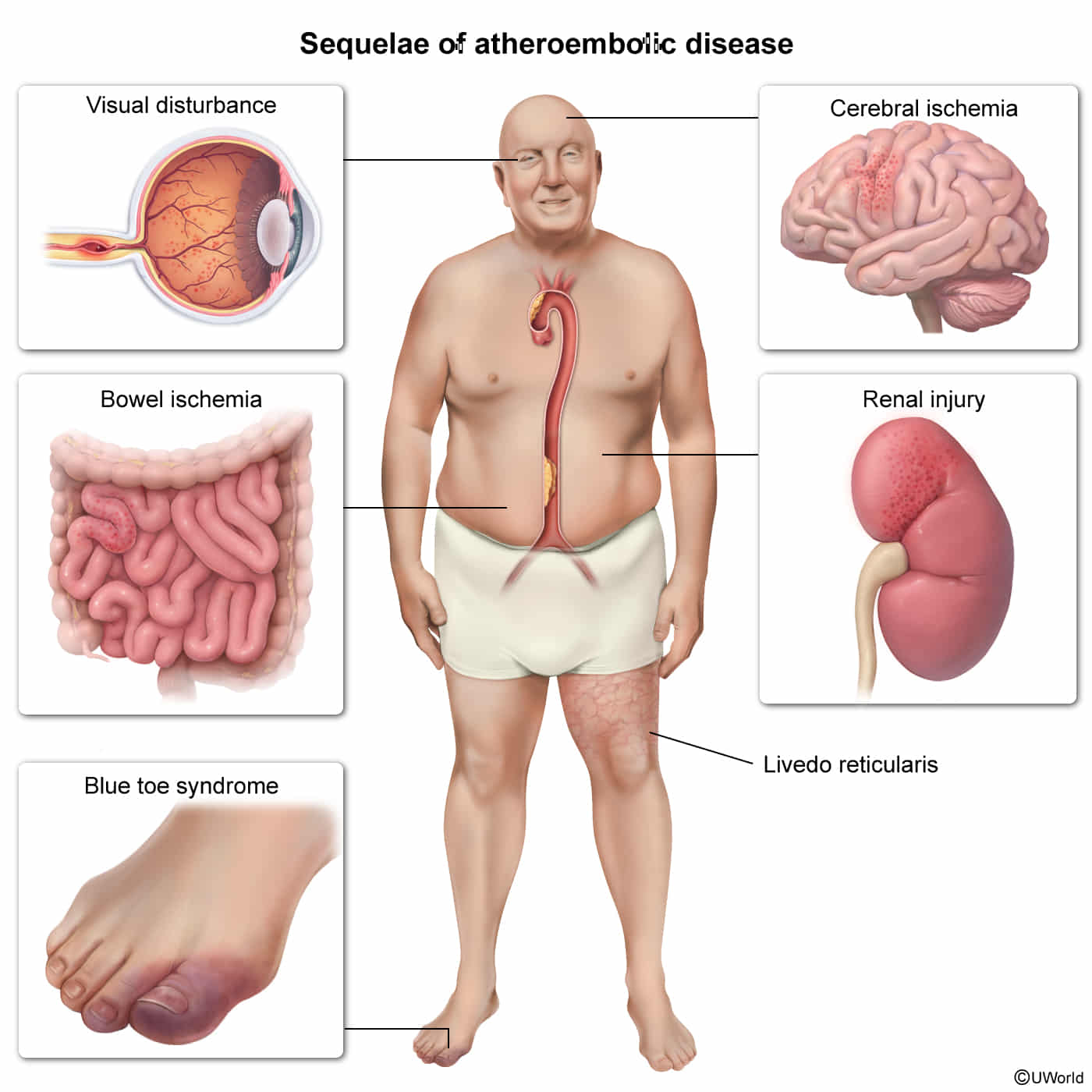
- Cutaneous: Livedo reticularis, “blue toe syndrome” (cyanotic toes w/ intact peripheral pulses), gangrene, skin ulcers. c

- Renal: Acute or subacute kidney injury (AKI) typically presenting 1-2 weeks post-procedure.
- Ocular: Hollenhorst plaques (bright yellow, refractile cholesterol plaques in retinal arterioles).
- GI: Intestinal ischemia (abd pain, bleeding).
- Neuro: TIA, stroke, amaurosis fugax.
- Systemic: Fever, myalgias, weight loss (mimics systemic vasculitis).
Diagnostics
- CBC with differential
- Leukocytosis, eosinophilia
- Anemia
- Thrombocytopenia
- Renal function tests: ↑ BUN, ↑ creatinine
- Urine studies: proteinuria, hematuria, eosinophiluria
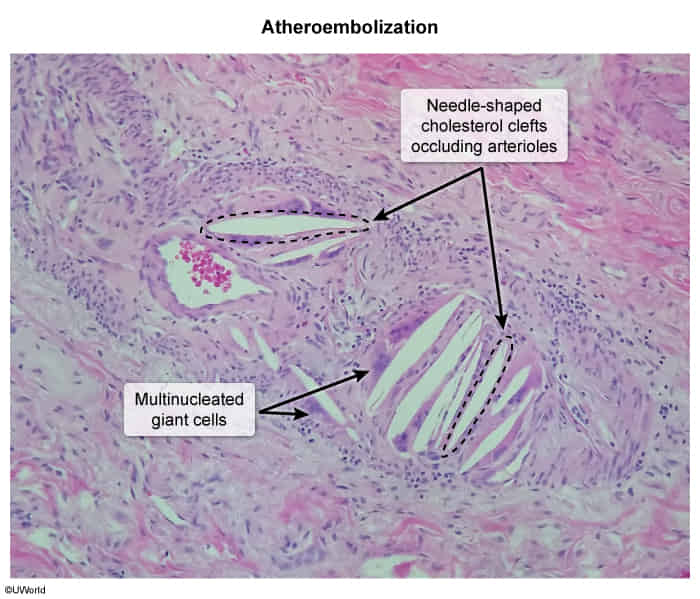
- Biopsy
- Amorphous, eosinophilic material in the vessel lumen
- Spindle-shaped spaces (cholesterol clefts)