Familial dyslipidemias
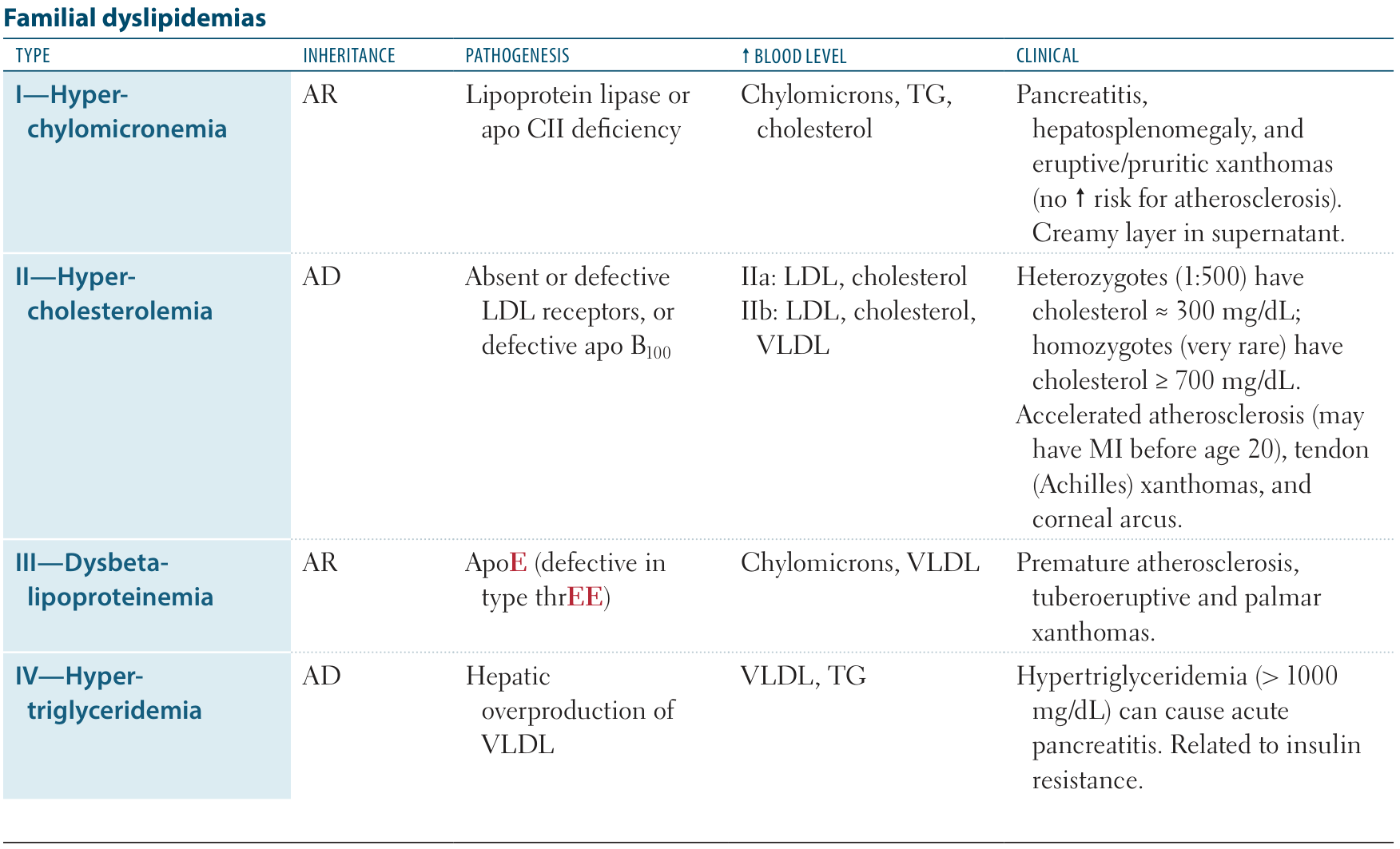
| Dyslipidemia | Protein defect | Elevated lipoproteins | Major manifestations |
|---|---|---|---|
| Familial chylomicronemia syndrome (type I) | Lipoprotein lipase, ApoC-2 | Chylomicrons (composed of TG, large) | Acute pancreatitis, Lipemia retinalis, Eruptive xanthomas |
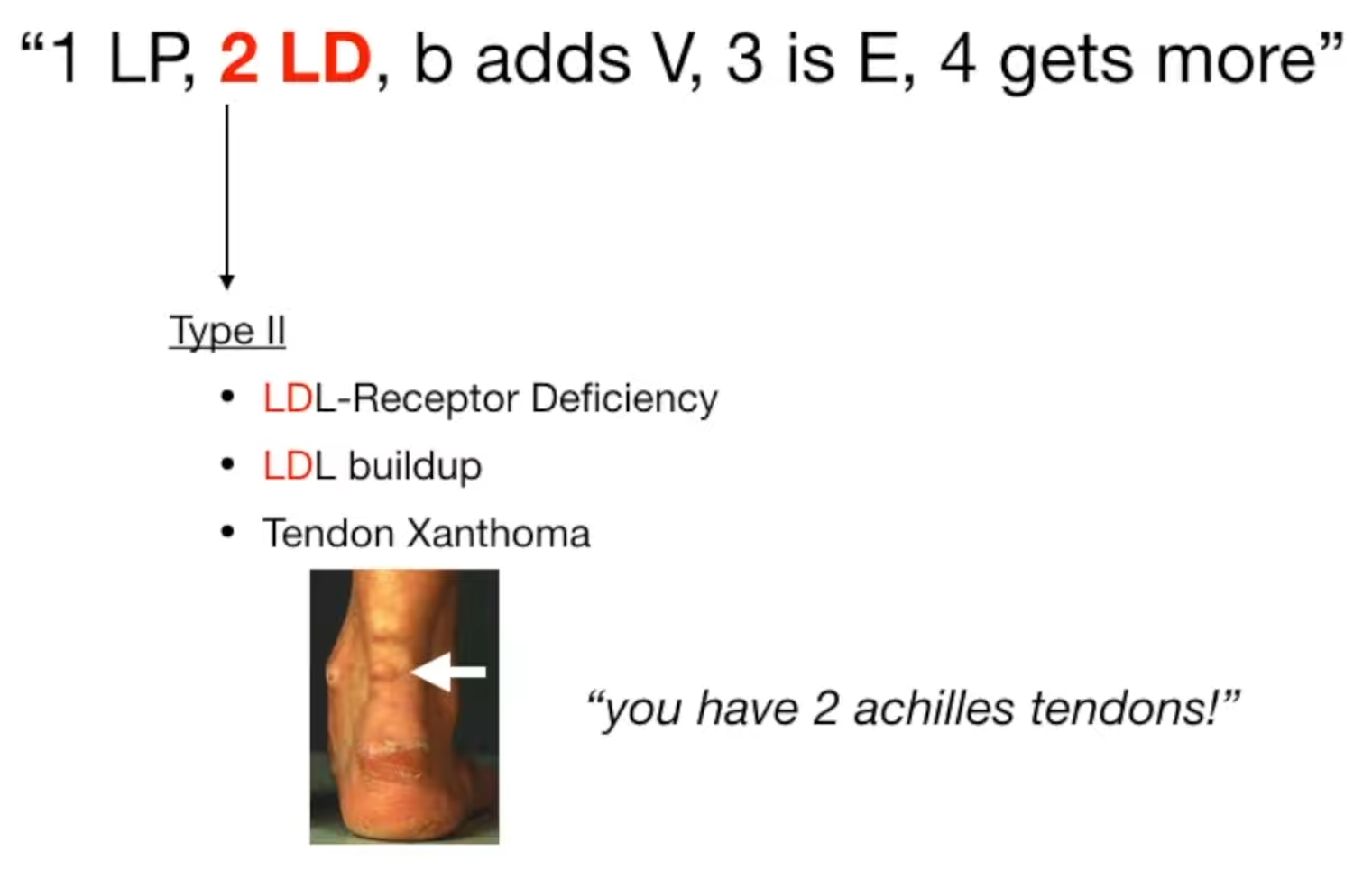
| Familial hypercholesterolemia (type II A) | LDL receptor, ApoB-100 | LDL (small and can enter vessel wall) | Premature Atherosclerotic cardiovascular disease, Tendon xanthomas, Xanthelasmas |
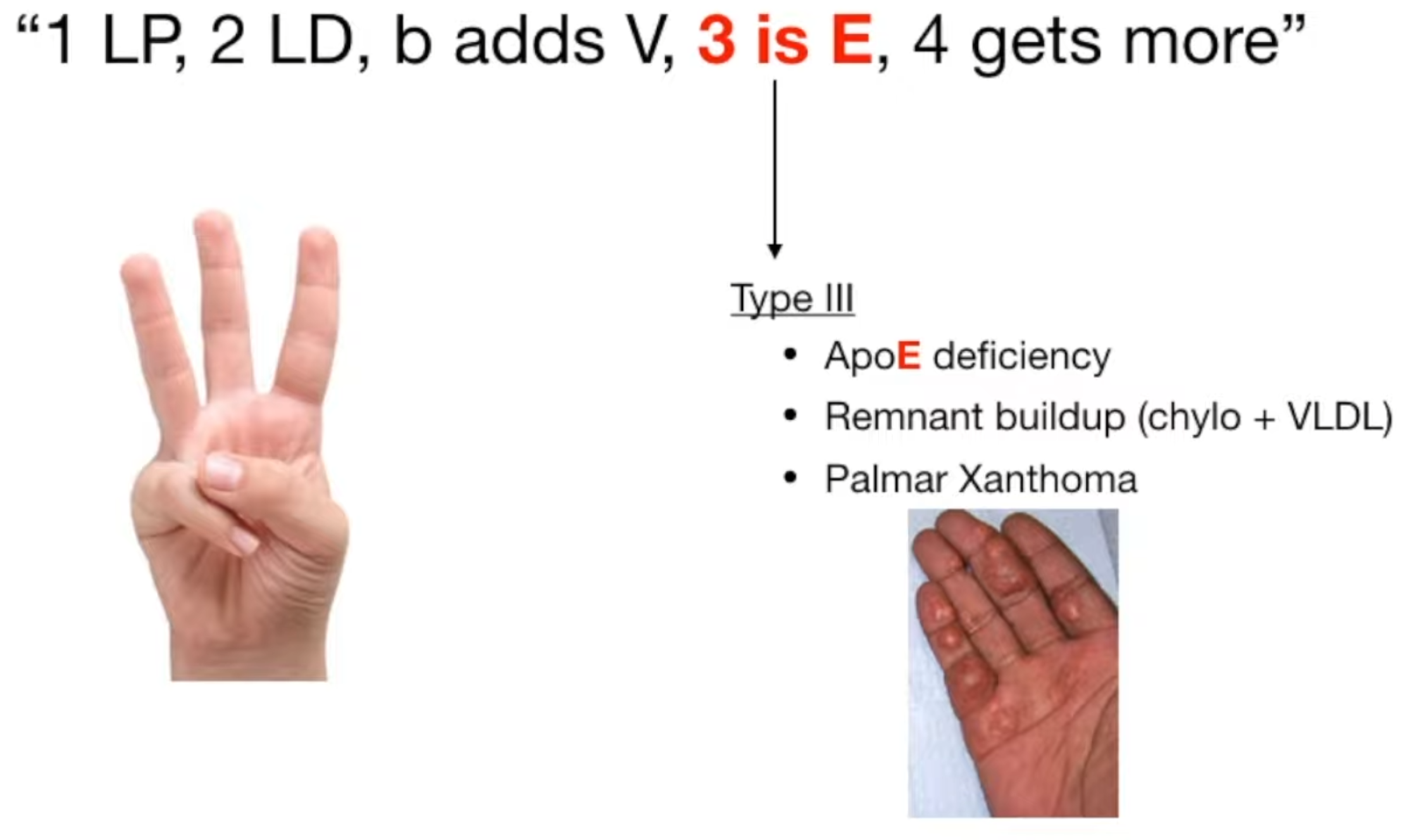
| Familial dysbetalipoproteinemia (type III) | ApoE | Chylomicron & VLDL remnants | Premature Atherosclerotic cardiovascular disease, Tuboeruptive & palmar xanthomas |
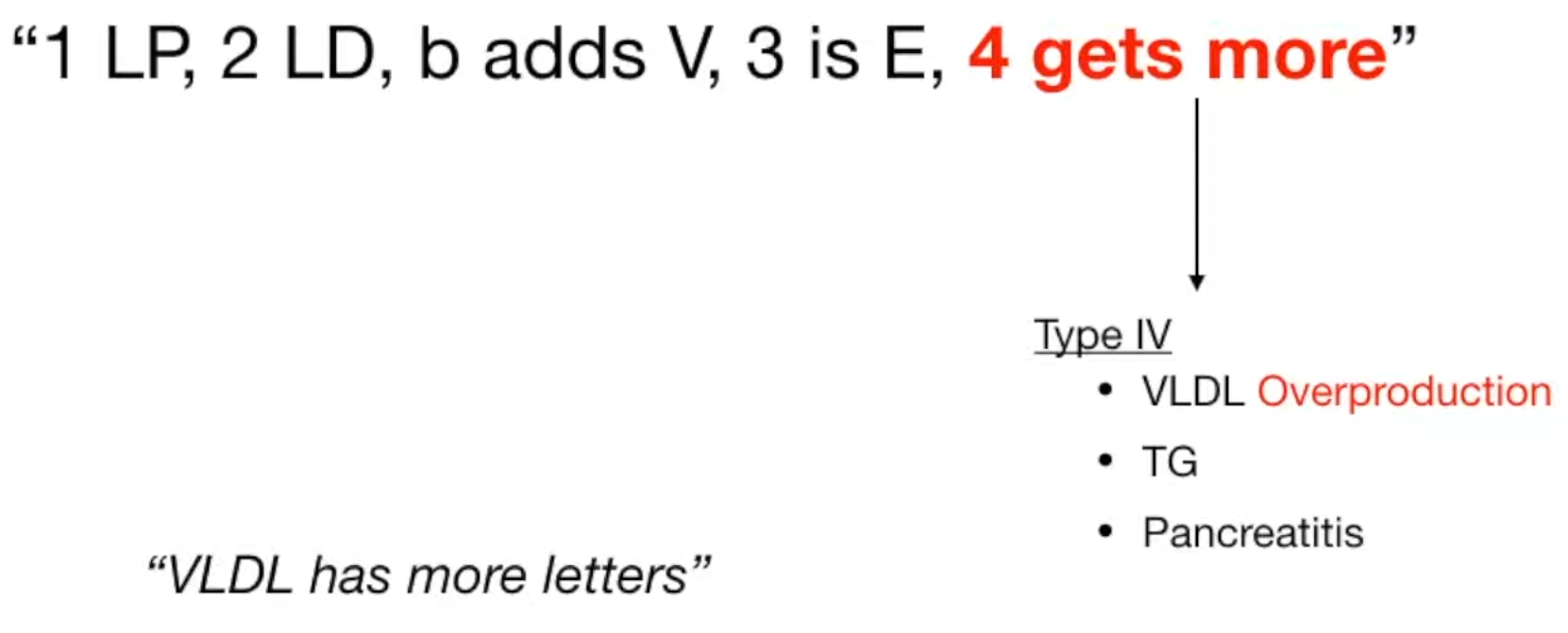
| Familial hypertriglyceridemia (type IV) | Polygenic | VLDL | Associated with coronary disease, pancreatitis & diabetes |
- Type II
- Premature Atherosclerotic cardiovascular disease, may lead to myocardial infarction at a very young age (< 20 years)
- Arcus lipoides corneae
- Tuberous/tendon xanthomas (especially the Achilles tendon) in type IIa
Treatment
- Goal: ASCVD risk reduction.
- The 4 Statin Benefit Groups (High-Yield):
- Clinical ASCVD (h/o ACS, MI, stable angina, stroke/TIA, PAD) → High-Intensity Statin.
- LDL ≥ 190 mg/dL (e.g., FH) → High-Intensity Statin.
- DM2, Age 40-75 → Moderate-Intensity Statin (Use High-Intensity if ASCVD risk ≥ 20% or multiple risk factors).
- No DM2, Age 40-75, LDL 70-189, ASCVD risk ≥ 7.5% → Moderate to High-Intensity Statin.
- Statin Intensities:
- High: Atorvastatin (40-80 mg), Rosuvastatin (20-40 mg). Lowers LDL ≥ 50%.
- Moderate: Atorvastatin (10-20 mg), Rosuvastatin (5-10 mg), Simvastatin (20-40 mg). Lowers LDL 30-49%.
- Hypertriglyceridemia Management:
- TG 150-499: Lifestyle modification (wt loss, ↓ EtOH, ↓ simple carbs). Statin if ASCVD risk indicates. c
- In this range, the primary threat is cardiovascular disease (CAD, stroke). The risk of acute pancreatitis only becomes significant when TG > 500 mg/dL (and especially > 1000 mg/dL).
- TG ≥ 500 (esp > 1000): Fibrates (Fenofibrate, Gemfibrozil) to prevent acute pancreatitis. Note: Statin is 2nd line here; primary goal is preventing pancreatitis, not just ASCVD.
- TG 150-499: Lifestyle modification (wt loss, ↓ EtOH, ↓ simple carbs). Statin if ASCVD risk indicates. c
- Adjunctive Therapies (If LDL target not met on max-tolerated statin):
- Ezetimibe: 1st-line add-on. ↓ cholesterol absorption.
- PCSK9 Inhibitors (Evolocumab, Alirocumab): 2nd-line add-on. Very effective, used in FH or recalcitrant ASCVD. SubQ injection.
Abetalipoproteinemia
- Etiology
- Deficiency of apolipoproteins (ApoB-48, ApoB-100) t
- Due to a mutation in the microsomal triglyceride transfer protein (MTTP) gene
- Pathophysiology
- Autosomal recessive disease
- Deficiency of chylomicrons, VLDL, and LDL (hypolipoproteinemia)
- Clinical features
- Early
- Steatorrhea
- Failure to thrive
- Fat malabsorption → fat-soluble vitamin deficiency
- Early
- Diagnostics
- Intestinal biopsy: Histology may reveal lipid-laden enterocytes.
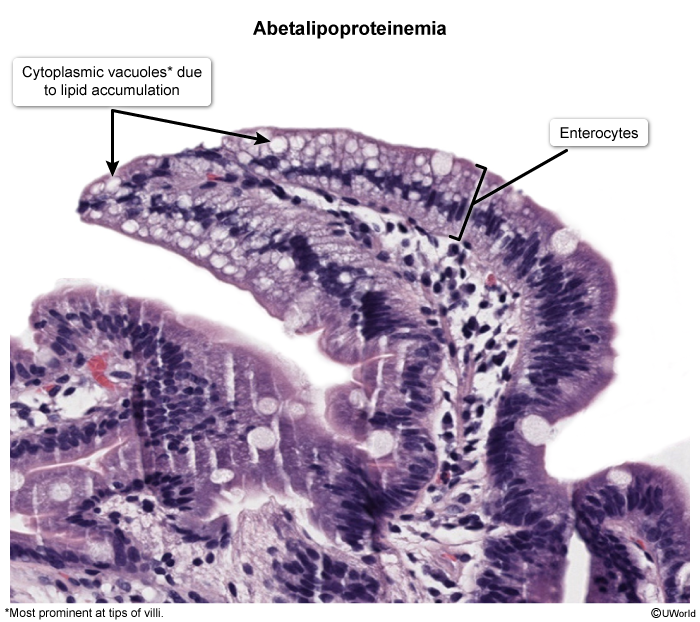
- Intestinal biopsy: Histology may reveal lipid-laden enterocytes.