Epidemiology
Etiology
Embolic strokes (∼ 20% of all strokes)
- Most commonly affect the middle cerebral artery (MCA)
- Likely cause multiple scattered infarcts in an asymmetric pattern within different major vascular territories (eg, middle and anterior cerebral artery)
Thrombotic strokes (∼ 40%)
- Large vessel Atherosclerotic cardiovascular disease (∼ 20%)
- Rupture of an atherosclerotic plaque and exposure of subendothelial collagen → formation of a thrombus
- Thrombus formation most commonly occurs at branch points in arteries (e.g., internal carotid artery bifurcation or where the MCA branches from the circle of Willis).
- Small vessel occlusion (e.g., lacunar infarct) (∼ 20%)
Global cerebral ischemia
- Systemic hypoperfusion
- Shock or bilateral large artery Atherosclerotic cardiovascular disease (e.g., of carotid arteries) → decreased effective oxygen delivery to the whole brain
- Common during cardiac surgeries
- Can result in watershed infarct
- Hypoglycemia: Repeated episodes of hypoglycemia (e.g., due to insulinoma) increase the risk of cerebral ischemia.
- Severe and/or chronic hypoxia: hypoxemia (e.g., due to respiratory arrest) → global tissue hypoxia in the brain
Stroke symptoms by affected region
Key Differentiating Principles:
- Cortical Signs: Present in cortical strokes, absent in lacunar strokes. Include aphasia, neglect, visual field cuts (hemianopia), gaze preference, and cortical sensory loss (e.g., agraphesthesia, astereognosis).
- Crossed Findings: Ipsilateral cranial nerve deficits with contralateral motor/sensory deficits strongly suggest a brainstem lesion.
Symptoms by Region:
-
Lacunar Syndromes (Deep Structures - Internal Capsule, Thalamus, Pons):
- Hallmark: NO cortical signs.
- Pure Motor: Contralateral weakness (face, arm, leg) ONLY.
- Pure Sensory: Contralateral numbness/paresthesia ONLY.
- Ataxic Hemiparesis: Ipsilateral ataxia + Contralateral weakness.
- Dysarthria-Clumsy Hand: Slurred speech + Contralateral face/hand weakness/clumsiness.
-
Brainstem Syndromes:
- Hallmark: Ipsilateral CN deficits + Contralateral tract deficits (“crossed findings”). Often vertigo, nystagmus, dysarthria, dysphagia.
- Midbrain (CN III, IV): Strokes here often involve the eyes. Look for a “down and out” pupil (CN III palsy) combined with weakness on the opposite side of the body.
- Pons (CN V, VI, VII, VIII): Strokes here often involve the face and horizontal eye movement. Look for facial weakness or numbness, inability to look to the side (abducens palsy), or “pinpoint pupils.”
- Medulla (CN IX, X, XI, XII): Strokes here often involve vital functions and swallowing. Look for hoarseness, dysphagia (difficulty swallowing), vertigo, and loss of pain/temperature sensation on the face.
-
Cerebellum:
- Hallmark: Ataxia (ipsilateral limb or truncal/gait), nystagmus, dysarthria (slurred speech). No hemiparesis. Headache/vomiting common.
-
Thalamus:
- Hallmark: Contralateral sensory loss (often all modalities). May have associated weakness, gaze deviation away from lesion (“wrong way eyes”), pupillary changes.
-
Cortex (Presence of Cortical Signs):
- Frontal Lobe: Contralateral weakness (leg > arm for ACA, arm/face > leg for MCA), gaze toward lesion, personality changes, expressive aphasia (dominant).
- Parietal Lobe: Contralateral sensory loss (incl. cortical type), neglect (non-dominant), Gerstmann syndrome (dominant: agraphia, acalculia, finger agnosia, L-R confusion).
- Temporal Lobe: Receptive aphasia (dominant), superior visual field cut (quadrantanopia).
- Occipital Lobe: Contralateral homonymous hemianopia (often with macular sparing).
-
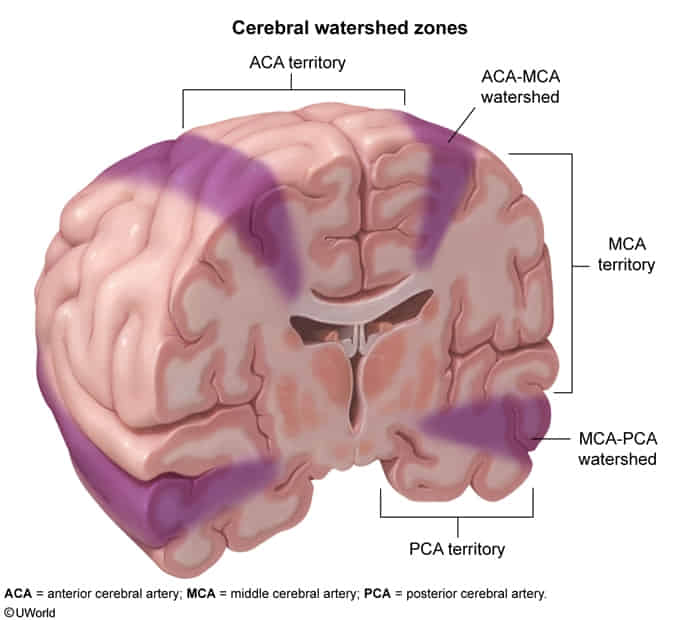
Watershed Areas (Hypoperfusion):
- ACA/MCA Zone: Proximal arm/leg weakness (“Man-in-the-barrel”).
- MCA/PCA Zone: Visual disturbances.
-
Retina (Central Retinal Artery Occlusion):
- Hallmark: Sudden, painless, complete unilateral vision loss.
Classifications
Tip
Most vulnerable: hippocampus (CA1 region), neocortex, cerebellum (Purkinje cells), watershed areas (“vulnerable hippos need pure water”). t
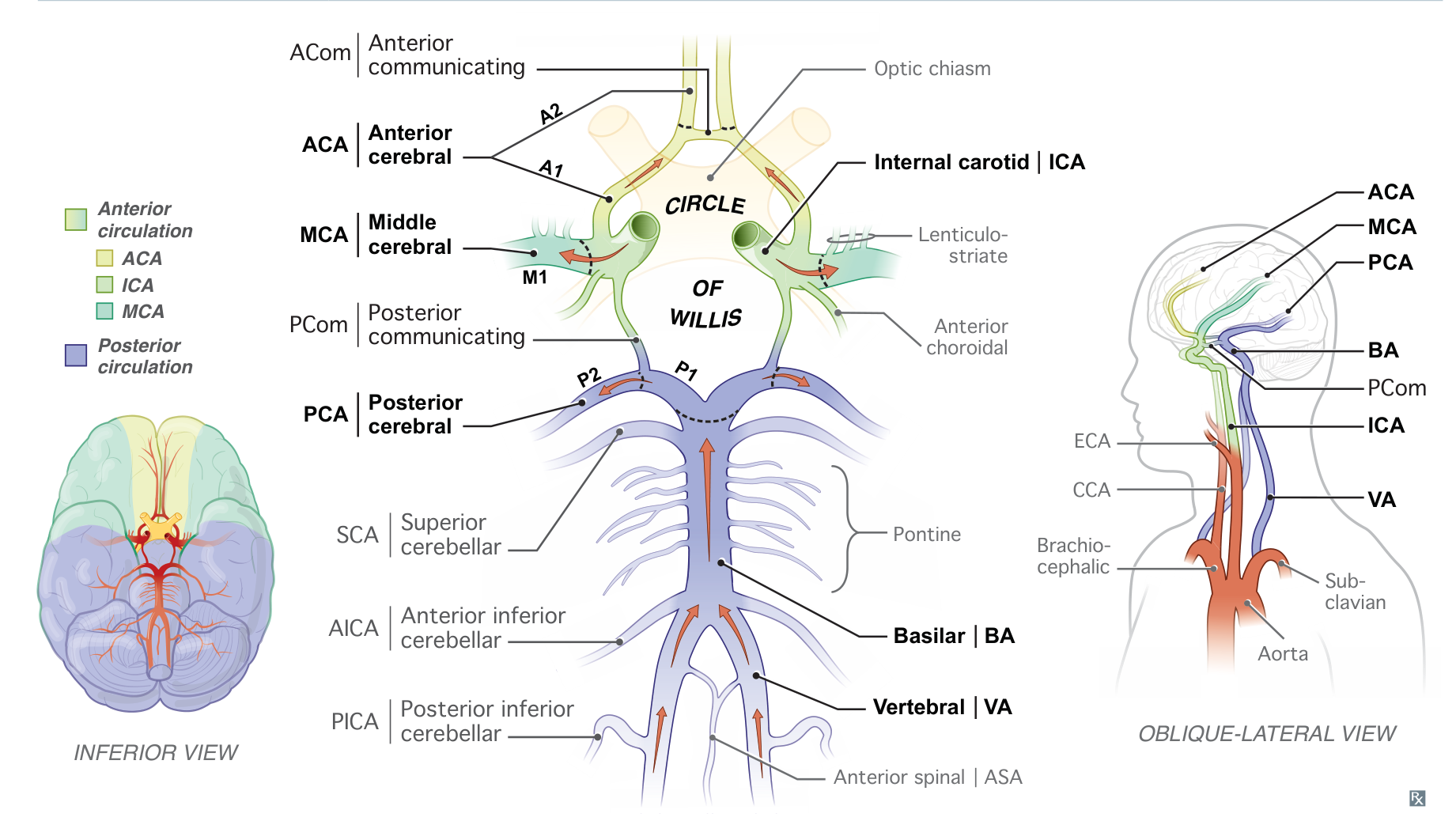
Anterior circulation
Posterior circulation
Posterior cerebral artery
A left posterior cerebral artery stroke can lead to alexia without agraphia in which someone is unable to read but can still write, speak, and listen.
Mnemonic
Someone cannot read letters if the post office workers have left for the day.
Anterior inferior cerebellar artery (Lateral pontine syndrome)
Lateral pontine syndrome is similar to lateral medullary syndrome but also involves facial paralysis and hearing loss.
Mnemonic
A stroke in the Anterior Inferior Cerebellar Artery messes up the fAICAl nerve.
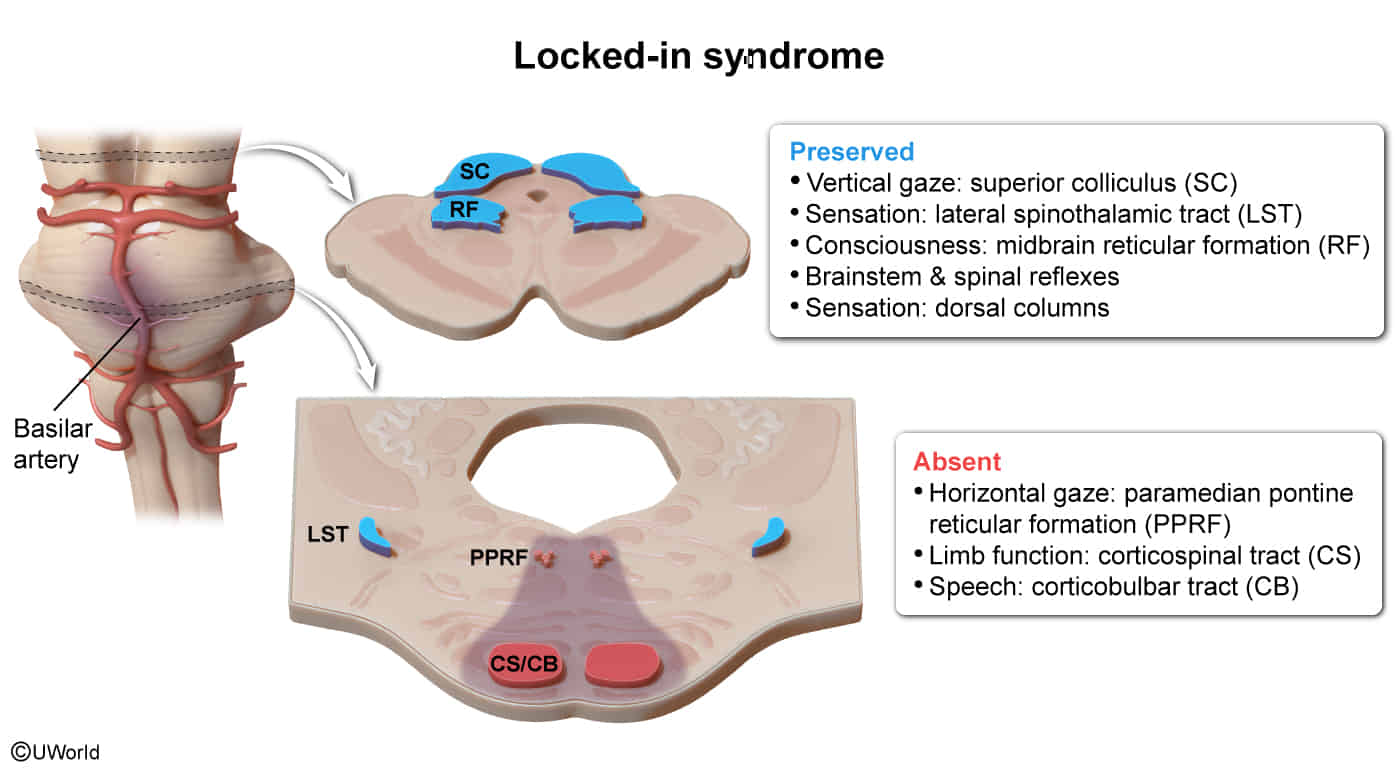
Basilar artery (Locked-in syndrome)
- Etiology
- Bilateral ventral pontine stroke (most common) t
- Ischemic stroke (thrombotic/embolic occlusion of the basilar artery)
- Hemorrhagic stroke
- Pontine demyelination (e.g., multiple sclerosis affecting the ventral pons, central pontine myelinolysis)
- Brain tumor or brain abscess affecting the ventral pons
- Bilateral ventral pontine stroke (most common) t
- Clinical features
- Caused by ischemic injury to the bilateral ventral pons
- Absent voluntary motor function of all limbs (quadriplegia) and oral structures (loss of speech) due to destruction of the cortical spinal and cortical bulbar pathways, which prevents cranial nerves or the limbs from receiving cortical signals.
- Absent horizontal eye movements. However, vertical eye movements and eyelid elevation are preserved because they are controlled in the rostral midbrain.
- Preserved consciousness because the midbrain reticular formation is spared. Behavioral arousal and sleep-wake cycles are also preserved because the diencephalon–upper brainstem arousal systems are unaffected.
- Preserved sensation because sensory pathways are not affected and preserved brainstem and spinal reflexes because they do not require cortical input.
Mnemonic
Locked-in syndrome (locked in the basement).
Anterior spinal artery
Medial medullary syndrome involves contralateral hemiplegia, contralateral epicritic numbness, and ipsilateral tongue weakness.
Mnemonic
“MM! These açaí (ASA-i) berries are so tasty I want to lick them!”
Posterior inferior cerebellar artery (Wallenberg syndrome, lateral medullary syndrome)
Attention
Posterior Inferior Cerebellar Artery (PICA) is a branch of Vertebral Artery, NOT Posterior Cerebral Artery (PCA).
Lateral medullary syndrome involves loss of protopathic sensation in the contralateral extremities and ipsilateral face, ipsilateral Horner’s syndrome, cerebellar signs, dysarthria, and dysphagia.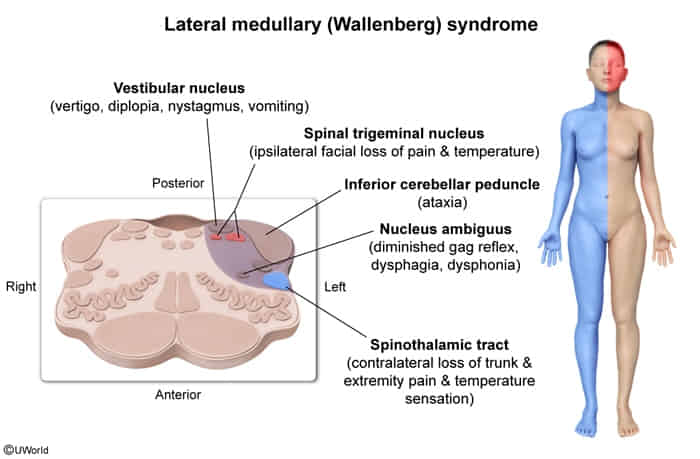
Mnemonic
PICA-chew: A Posterior Inferior Cerebellar Artery stroke makes it so you can’t chew.
Pathophysiology
- Mechanism: Ischemia ↓ ATP Na⁺/K⁺ pump failure cytotoxic edema + glutamate excitotoxicity.
- Membrane depolarization massive Glutamate release Activates postsynaptic NMDA receptors NMDA activation opens Ca2+ channels massive Ca2+ influx Ca2+ activates degradative enzymes (proteases, phospholipases) Cell Death.
- 12–24 hours: Red neurons (eosinophilic cytoplasm, pyknotic nuclei).
- 1–3 days: Neutrophil infiltration (necrosis begins).
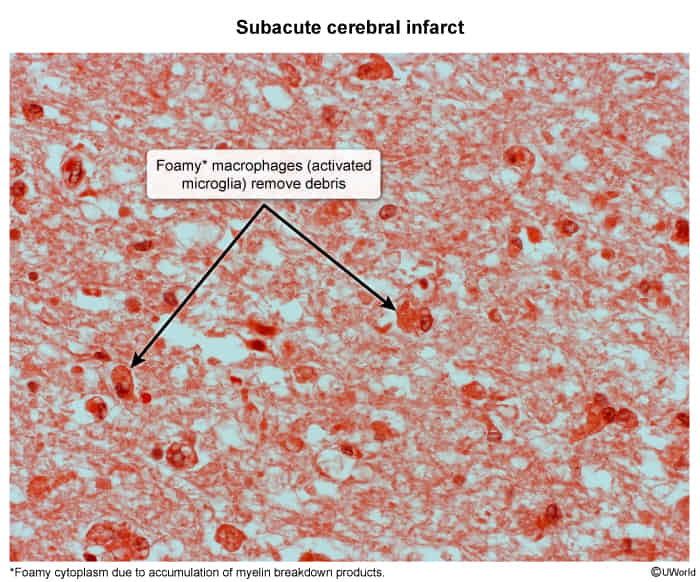
- 3–7 days: Macrophage infiltration (microglia).
- 1–2 weeks: Reactive Gliosis (astrocytes) + vascular proliferation.
- >2 weeks: Glial Scar surrounds cystic cavity (Liquefactive necrosis).
Hierarchy of Vulnerability (Most to Least)
- Hippocampus: CA1 Pyramidal cells (Most sensitive overall). t
- Result: Anterograde amnesia.
- Cerebellum: Purkinje cells.
- Result: Ataxia.
- Neocortex: Pyramidal cells (Layers 3, 5, 6).
- Result: Laminar necrosis.
- Watershed Zones (Hypoperfusion)
- ACA-MCA Border: Due to systemic hypotension (shock).
- Result: “Man-in-a-barrel” syndrome (proximal arm/leg weakness).
Clinical features
Subtypes and variants
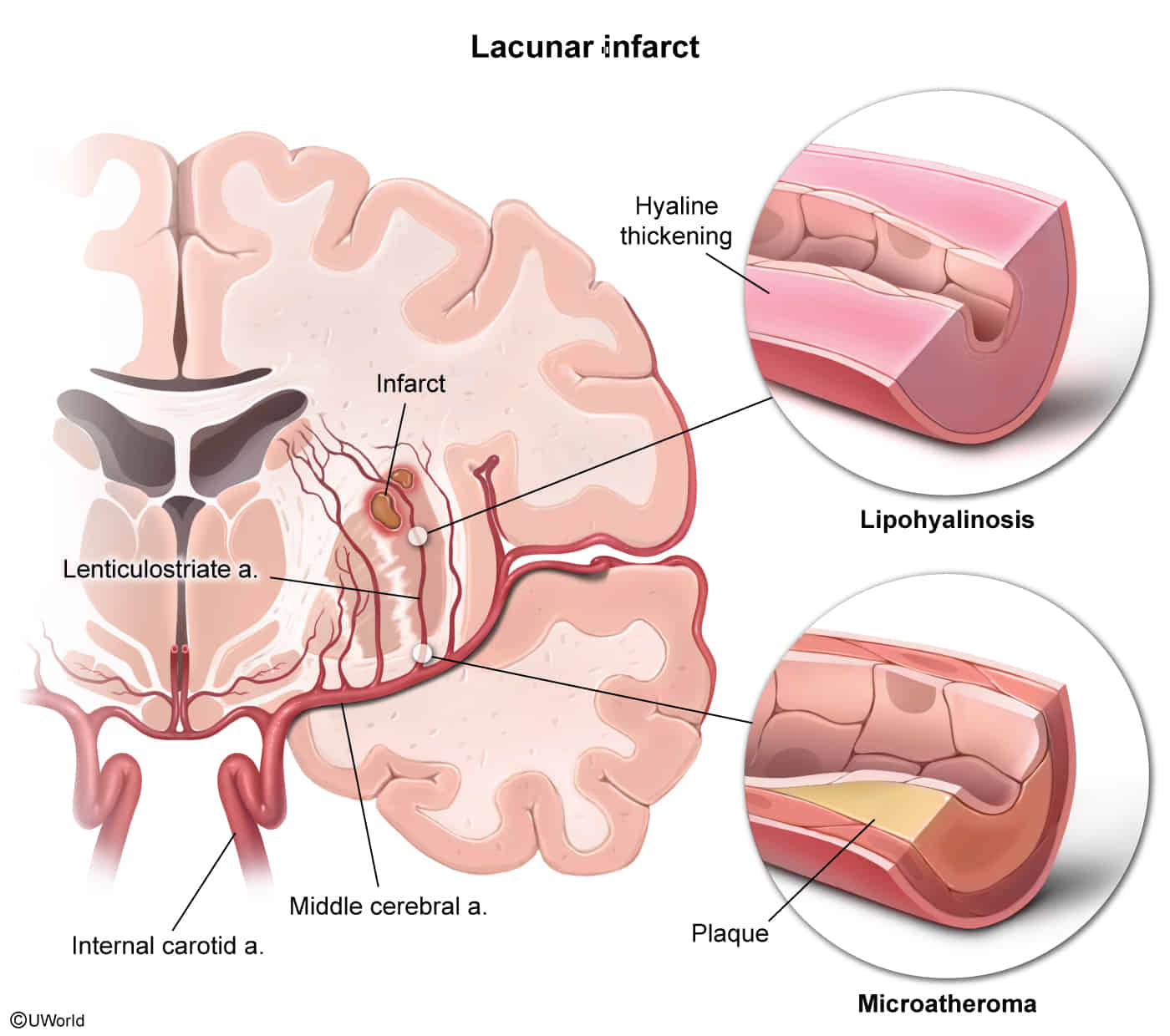
Lacunar infarction
- Definition: noncortical infarcts characterized by the absence of cortical signs (e.g., no aphasia, hemianopsia, agnosia, apraxia)
- Etiology
- Most common: chronic hypertensive vasculopathy → lipohyalinosis of the small vessels → occlusion of small, penetrating arteries (e.g., lenticulostriate artery) → lacunar stroke resulting in specific lacunar syndromes
- Most common: chronic hypertensive vasculopathy → lipohyalinosis of the small vessels → occlusion of small, penetrating arteries (e.g., lenticulostriate artery) → lacunar stroke resulting in specific lacunar syndromes
- Risk factors
- Clinical features
- Pure motor stroke
- Location
- Posterior limb of the internal capsule (most common)
- May also involve striatum, corona radiata, basal pons, medial medulla
- Often caused by occlusion of the lenticulostriate artery
- Clinical features
- Contralateral hemiparesis of the face, arm, and leg (causes circumduction gait)
- No sensory impairment
- Most common type of lacunar stroke (> 50%)
- Location
- Pure motor stroke
Tip
If an infarction causes abnormalities in multiple body parts (e.g., legs + arms + face), it is unlikely to be a cortical infarction, because the cortical areas corresponding to different parts are supplied by different vessels. A thalamic (sensory) or internal capsule (motor) infarction is more likely.
Watershed infarct
- Definition: border-zone infarct in the region between the territory of two major arteries that supply the brain (watershed area)
- Etiology: sudden decrease in blood pressure or cessation of blood flow through both vessels → ischemia in the susceptible region between two vascular territories
- Systemic hypotension (e.g. cardiogenic shock, septic shock)
- Clinical features
- Signs of systemic hypoperfusion (e.g., tachycardia, low blood pressure, pallor, sweating)
- Diffuse neurological deterioration
- PCA-MCA watershed region: bilateral visual loss (cortical blindness)
- ACA-MCA watershed region: proximal limb weakness with sparing of the face, hands, and feet (“man-in-the-barrel syndrome”)
Diagnostics
Pathology
- 12-24 hours
- Microscopic: Red neurons (eosinophilic cytoplasm, pyknotic nuclei, loss of Nissl substance)
- Macroscopic: No significant changes
- 24-72 hours
- Microscopic: Neutrophilic infiltration
- Macroscopic: No significant changes
- 3-7 days
- Microscopic: Macrophage/microglia infiltration & phagocytosis begins
- Macroscopic: No significant changes
- Microscopic: Macrophage/microglia infiltration & phagocytosis begins
- 1-2 weeks
- Microscopic: Reactive gliosis (astrocytes) & vascular proliferation around the necrotic area t
- Gliosis (specifically reactive astrocytosis) is the central nervous system’s equivalent of scar formation (fibrosis) seen in peripheral tissues.
- Macroscopic: Liquefactive necrosis (continues 1 week-1 month)
- Microscopic: Reactive gliosis (astrocytes) & vascular proliferation around the necrotic area t
- >2 weeks
- Microscopic: Glial scar formation
- Macroscopic: Cystic area surrounded by dense glial fibers (develops after >1 month)