Etiology
- Infection of the endocardium, most commonly affecting heart valves.
- Pathogenesis: Endothelial damage → sterile platelet-fibrin thrombus (nonbacterial thrombotic endocarditis) → transient bacteremia seeds the thrombus → vegetation formation.
Pathogens
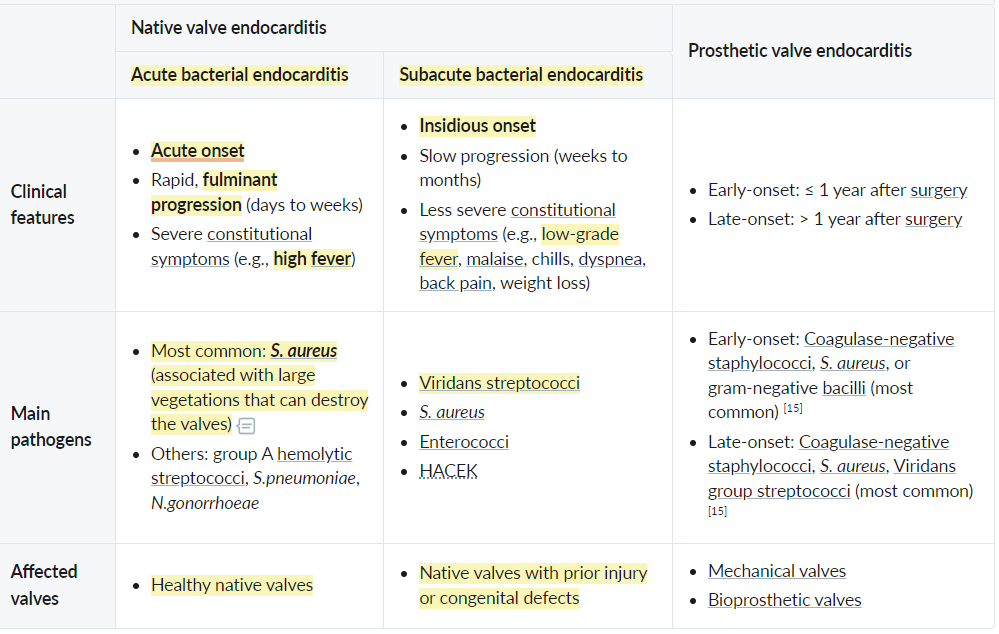
- ** S. aureus **: Most common cause overall, especially in IV drug users (IVDU), healthcare-associated infections, and acute, aggressive presentations.
- ** Viridans group streptococci ** (S. sanguinis): Associated with poor dentition and recent dental procedures; typically causes subacute IE on previously damaged valves.
- ** S. bovis (S. gallolyticus) **: Strongly associated with colon cancer; a workup for colonic malignancy is required if isolated.
- Enterococci (E. faecalis): Common after GU/GI procedures and in nosocomial settings.
- Coagulase-negative staphylococci (S. epidermidis): Associated with prosthetic valves, especially within the first year of placement.
- HACEK organisms: Haemophilus, Aggregatibacter, Cardiobacterium, Eikenella, Kingella. Part of normal oral flora, associated with culture-negative endocarditis.
- Fungi (Candida, Aspergillus): Seen in immunocompromised patients, IVDU, and after prolonged antibiotic therapy.
Risk factors for infective endocarditis
- Cardiac conditions
- Acquired valvular disease (e.g., Mitral valve prolapse (most common), rheumatic fever, aortic stenosis, degenerative valvular disease)
- Prosthetic heart valves
- Congenital heart defects (e.g., VSD, bicuspid aortic valve)
- Noncardiac risk factors
- Poor dental status
- Dental procedures
- Nonsterile venous injections (e.g., in IV drug use)
- Intravascular devices
- Surgery
Pathophysiology
- Pathogenesis
- Damaged valvular endothelium → exposure of the subendothelial layer → adherence of platelets and fibrin → sterile vegetation (microthrombus)
- Localized infection or contamination → bacteremia → bacterial colonization of vegetation → formation of fibrin clots encasing the vegetation → valve destruction with loss of function (valve regurgitation)
- Clinical consequences
- Bacterial vegetation → bacterial thromboemboli → vessel occlusion → infarctions
- Emboli can lead to metastatic infections of other organs.
Classifications
 Coagulase-negative staphylococci (CoNS): Staphylococcus epidermidis, Staphylococcus saprophyticus
Coagulase-negative staphylococci (CoNS): Staphylococcus epidermidis, Staphylococcus saprophyticus
Clinical features
Cardiac manifestations
- Development of a new heart murmur or change in a preexisting murmur
- Tricuspid valve regurgitation
- Holosystolic murmur that is loudest at the left sternal border
- Seen in persons who inject drugs, immunocompromised individuals, patients with congenital heart disease, and patients with instrumentation in the right heart (e.g., central venous catheters)
- Aortic valve regurgitation: early diastolic murmur that is loudest at the left 3rd and 4thintercostal spaces and along the left sternal border
- Mitral valve regurgitation: holosystolic murmur that is loudest at the heart’s apex and radiates to the left axilla
- Tricuspid valve regurgitation
Extracardiac manifestations of IE
- Pulmonary manifestations: caused by septic emboli resulting from tricuspid valve involvement
- Signs of pulmonary embolism (e.g., dyspnea)
- Signs of pulmonary infection, e.g., multifocal pneumonia, lung abscess, and/or empyema.
Diagnostics
- Initial Step: Obtain 3 sets of blood cultures from different venipuncture sites prior to starting empiric Abx.
- Key Labs: Normocytic anemia, leukocytosis, ↑ ESR/CRP, hematuria/proteinuria (if GN present). ECG (monitor for new AV block).
- Imaging:
- Initial: Transthoracic echocardiogram (TTE).
- Confirmatory/Best: Transesophageal echocardiogram (TEE). Superior sensitivity. Indicated if TTE is negative but suspicion is high, or for assessing prosthetic valves/complications (abscess). c
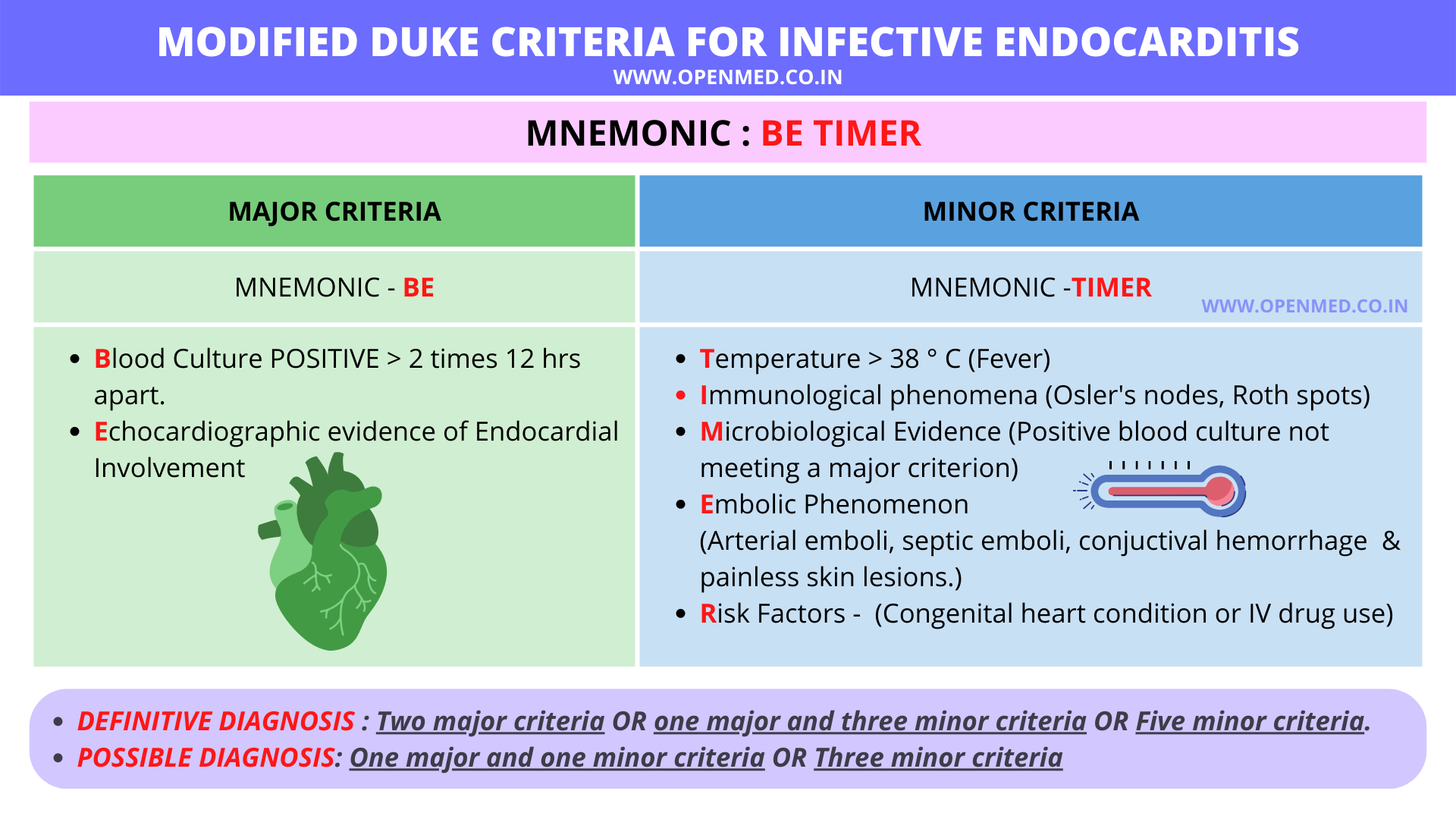
- Major Criteria: (+) Blood cx for typical org x2, (+) Echo (vegetation, abscess, new partial dehiscence of prosthetic valve), or new valvular regurgitation.
- Minor Criteria: Predisposing condition/IVDU, Fever > 38°C, Vascular phenomena, Immunologic phenomena, (+) Blood cx not meeting major criteria.
 vs
vs 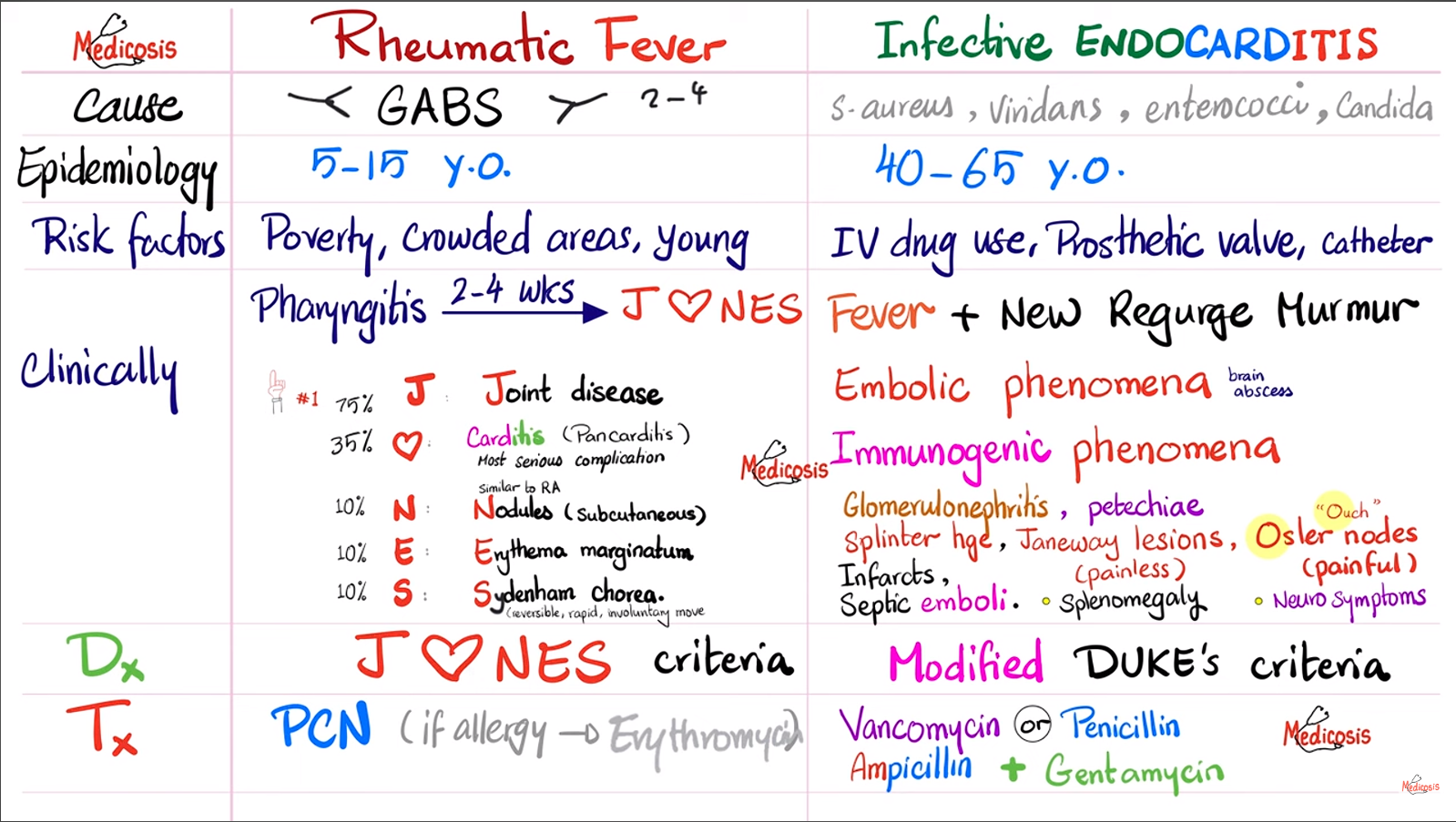
Treatment
- Hemodynamic Stabilization: ABCs, manage acute HF if present.
- Empiric Abx (After 3 sets of blood cx):
- Native valve: IV Vancomycin (covers MRSA) + Ceftriaxone (covers HACEK/Strep).
- Prosthetic valve: IV Vancomycin + Gentamicin + Cefepime/Carbapenem (add Rifampin later once organism known/staph confirmed).
- Targeted Abx (Based on Cx/Sensitivities, usually 4-6 weeks IV):
- MSSA: Nafcillin or Oxacillin.
- MRSA: Vancomycin.
- Viridans Strep: Penicillin G or Ceftriaxone.
- Surgical Valve Replacement (Indications for early surgery):
- Severe heart failure (refractory). c
- Cardiogenic shock / Hemodynamic instability.
- Perivalvular abscess / New heart block.
- Persistent bacteremia > 7 days despite appropriate IV Abx.
- Fungal or highly resistant organisms.
- Recurrent emboli.
- Prophylaxis (for future procedures):
- Who: ONLY highest risk (prosthetic valve, prior IE, unrepaired cyanotic CHD, repaired CHD w/ residual defect, cardiac transplant w/ abnormal valve).
- When: ONLY high-risk procedures (dental work w/ gingival manipulation, resp tract incisions, infected skin/MSK procedures). Not for routine GI/GU procedures. c
- What: Amoxicillin PO (or Ampicillin/Ceftriaxone IV). Clindamycin/Azithromycin if PCN allergic.
Complications
Perivalvular abscess
- Epidemiology & Risk Factors
- High-risk complication of Infective Endocarditis (IE); occurs in ~30-40% of cases.
- Prosthetic valves (PVE) > Native valves (NVE).
- Location: Aortic valve (most common) > Mitral valve.
- Clinical Features
- Persistent fever/bacteremia despite appropriate IV Abx therapy.
- New-onset conduction abnormality: Pathognomonic for extension of infection into the septum/conduction system. c
- Symptoms of worsening Heart Failure (HF): Dyspnea, orthopnea, pulmonary edema.
- New or changing heart murmur (e.g., new AR murmur in aortic root abscess).
- Diagnosis
- Initial Step: EKG. Look for new 1st-degree AV block, bundle branch block, or complete heart block.
- Confirmatory/Best Imaging: Transesophageal Echocardiogram (TEE).
- Sensitivity for abscess: TEE (>90%) vs. TTE (<40%).
- Necessary to visualize perivalvular extension, vegetations, or fistula.
- Blood Cultures: Persistently (+) despite therapy.
- Differential Diagnostics
- Uncomplicated IE: Fever/murmur but no conduction delay; responds to Abx.
- Acute Rheumatic Fever: Post-strep, Jones criteria, usually younger pts, migratory polyarthritis.
- Myocarditis: Viral prodrome, diffuse ST changes, elevated troponin, global LV dysfunction.
- Aortic Dissection: Sudden tearing chest pain, asymmetric BPs, widened mediastinum on CXR.
- Management
- Surgical Intervention (Essential): Indicated for almost all perivalvular abscesses (debridement + valve replacement).
- Medical Therapy: High-dose IV Abx (tailored to culture/sensitivities) for 6+ weeks.
- Supportive: Stabilization of hemodynamics, management of HF symptoms (diuretics).