Epidemiology
Etiology
Pathophysiology
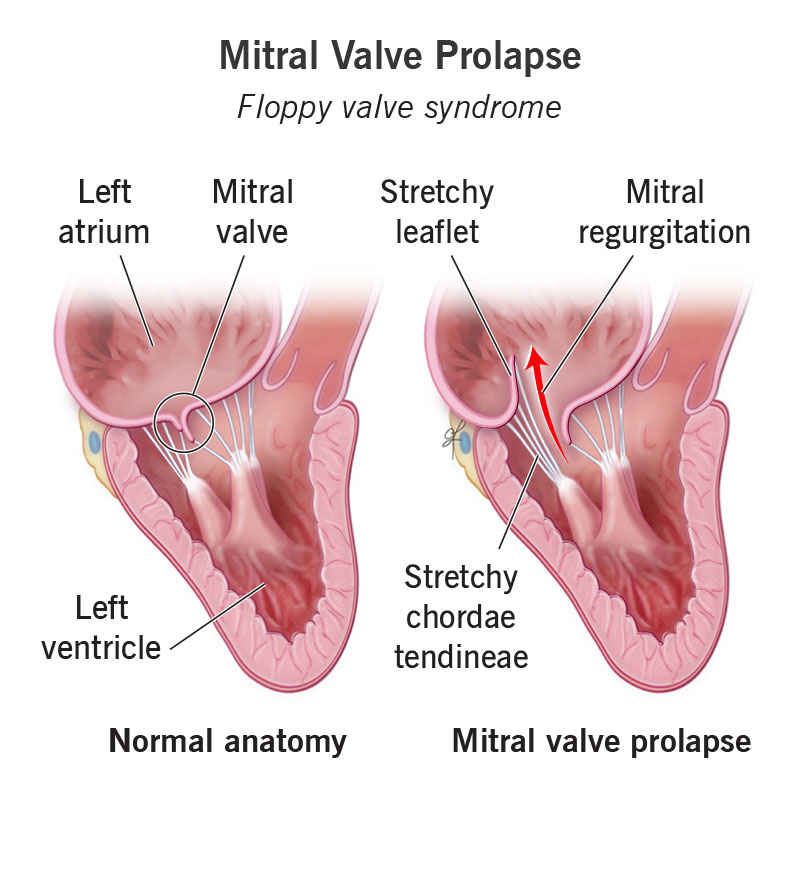
Myxomatous degeneration of the mitral valve leaflets and chordae tendineae is the primary cause, leading to redundant , thickened, and “floppy” valve tissue. This causes the leaflets to bulge (prolapse) into the left atrium during systole.It’s the most common cause of primary mitral regurgitation (MR) Can be an isolated finding or associated with connective tissue diseases like Marfan syndrome , Ehlers-Danlos syndrome , and osteogenesis imperfecta .
Clinical features
Auscultation
Classic Finding: Mid-systolic non-ejection click (caused by sudden tensing of chordae tendineae as leaflets prolapse into LA).Murmur: Followed by a late systolic murmur (due to Mitral Regurgitation).Location: Best heard at the Apex .Dynamic Maneuvers (High-Yield)
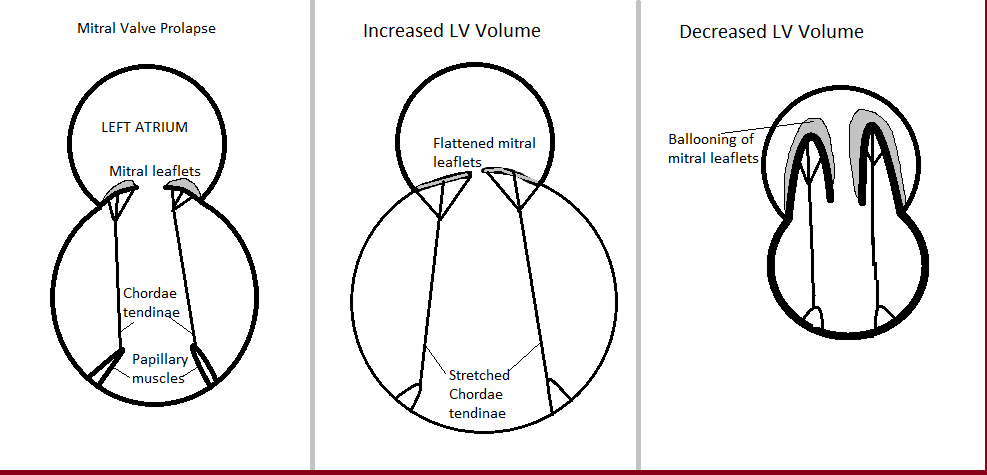
Changes in Left Ventricular (LV) volume alter the timing of the click and murmur duration.
↓ Preload (Standing, Valsalva phase II):
Mechanism: ↓ LV volume → Critical leaflet overlap size reached sooner.Result: Click moves earlier (closer to S1) → Murmur becomes longer .
↑ Preload (Squatting, Passive Leg Raise):
Mechanism: ↑ LV volume → Takes longer for leaflets to prolapse.Result: Click moves later (closer to S2) → Murmur becomes shorter .
↑ Afterload (Handgrip):
Mechanism: ↑ Systemic vascular resistance → ↑ Backflow pressure.Result: Murmur ↑ intensity (louder) and duration (Contrast with HOCM, which ↓ with handgrip).
Diagnostics
Treatment