Progressive weakening of arterial wall due to elastin degradation and inflammation; atherosclerosis leads to oxidative stress and matrix metalloproteinase activation
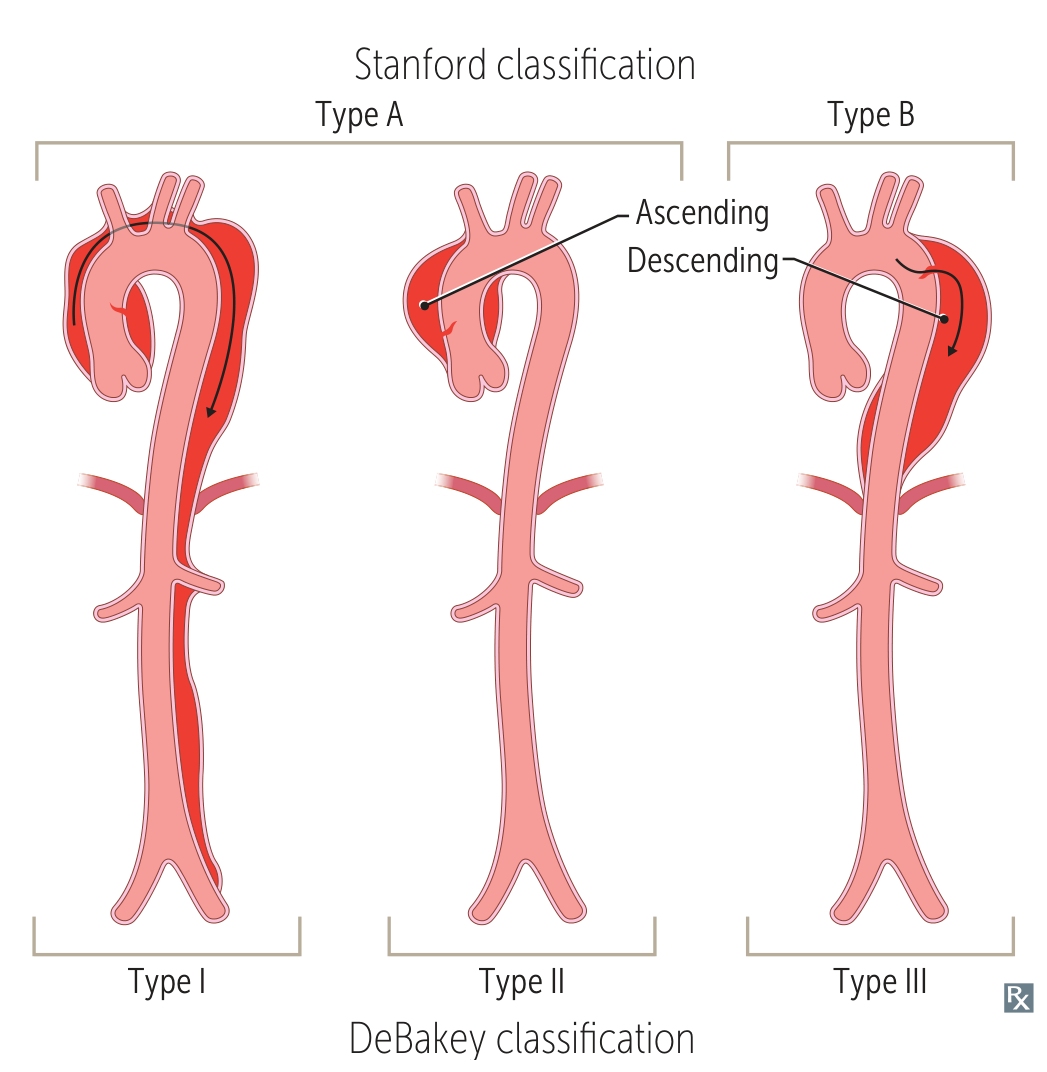
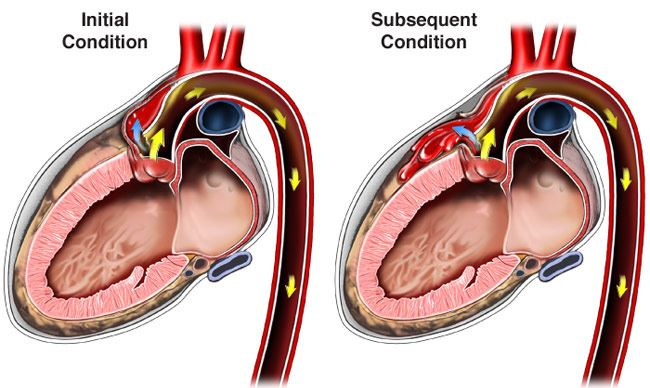
Intimal tear allows blood to enter media, creating false lumen; can be triggered by hypertensive crisis or inherited connective tissue disorders
Onset
Gradual
Sudden, acute
Pain
Usually asymptomatic; may have dull abdominal/back pain
Severe, tearing chest/back pain; migrating
Physical Exam
Pulsatile abdominal mass
Unequal pulses, BP differences between arms
Complications
Rupture with hemorrhagic shock
Organ ischemia, tamponade, aortic rupture
Imaging
Ultrasound, CT with contrast
CT angiogram, TEE
Treatment
Endovascular repair (EVAR) or open surgery if >5.5cm
Emergency surgery (Type A), medical management (Type B)
Mortality
80% if ruptured; 5% with elective repair
50% at 48h without treatment (Type A)
Clinical features
Pain: Sudden onset, severe, “tearing” or “ripping” quality. Radiates to back (interscapular).
PE:
BP Asymmetry: >20 mmHg diff in SBP between arms.
Pulse Deficit: Weak/absent carotid, radial, or femoral pulses. c
AR Murmur: New early diastolic decrescendo murmur (if dissection involves aortic root). c
Horner Syn: Ptosis/miosis/anhidrosis (compression of symp chain).
Diagnostics
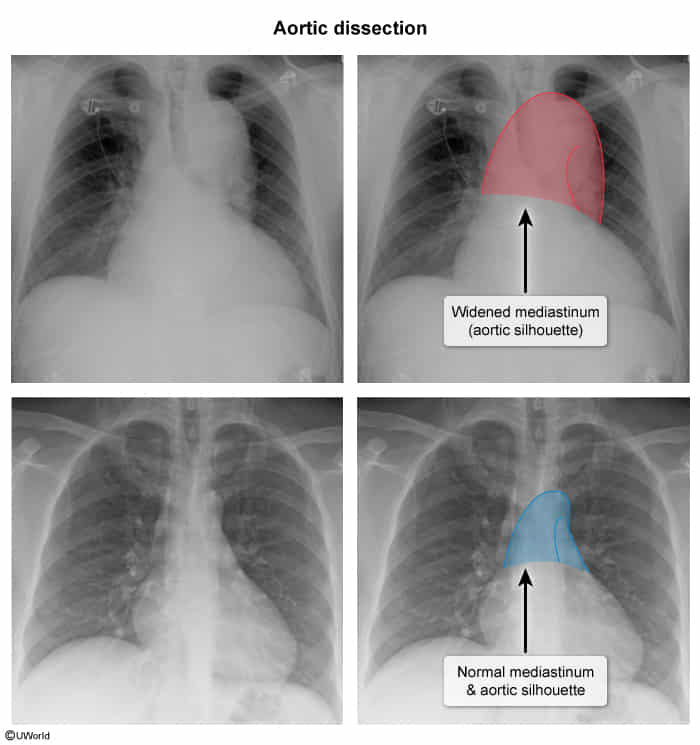
Chest X-ray (CXR): Often the first imaging study; may show a widened mediastinum (>8 cm).
CT Angiography (CTA): Gold standard for diagnosis in hemodynamically stable patients. Shows intimal flap and true/false lumens.
Transesophageal Echocardiogram (TEE): Best test for hemodynamically unstable patients c ; can be done at the bedside. Also excellent for evaluating aortic regurgitation and pericardial effusion/tamponade.
ECG: May be normal or show non-specific ST/T wave changes. Can show STEMI if a coronary artery is occluded (esp. the RCA).c
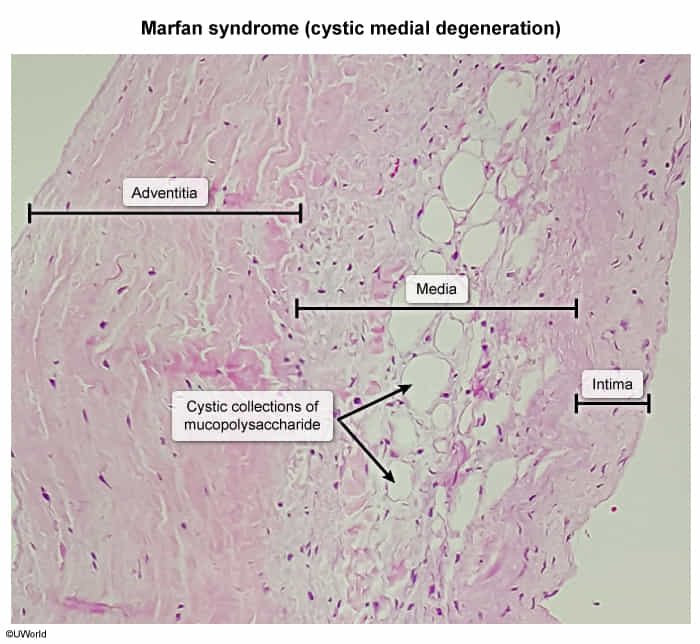
Pathology
Cystic medial degeneration: a degeneration (necrosis) of large blood vessels such as the aorta.
Pulse/BP deficit (>20mmHg diff), new AR murmur, focal neuro deficits
ECG / CXR
ST changes, ↑ Troponins / Normal CXR
Normal ECG / Widened mediastinum
Diagnostic
ECG (initial) → Angiography (definitive)
CTA (stable) or TEE (unstable/renal injury)
Acute Rx
ASA, Heparin, PCI
IV β-blocker (Esmolol/Labetalol) to ↓ HR/BP → Surg (Type A) or Meds (Type B)
WARNING!
Exclude AD before giving anticoagulants
FATAL if given ASA/Heparin/tPA
Treatment
Stabilize / Medical Management (Step 1 for ALL pts):
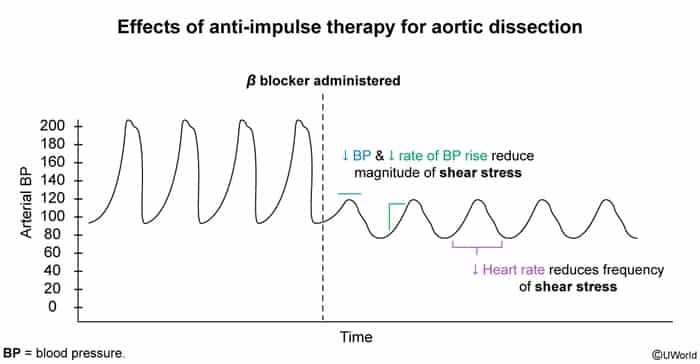
1st Line: IV Beta-blockers (e.g., Labetalol, Esmolol) to strictly ↓ HR (<60 bpm) and ↓ LV dP/dt (shearing force). t
2nd Line: Add IV vasodilator (e.g., Nitroprusside) to ↓ SBP (target 100-120 mmHg) ONLY AFTER HR is controlled by beta-blockade (prevents reflex tachycardia, which worsens dissection).
Adequate analgesia (IV Morphine) to ↓ sympathetic output.
Definitive Therapy:
Type A (Ascending): Urgent open surgical repair.
Type B (Descending) Uncomplicated: Medical management (strict BP/HR control).
The descending aorta supplies the intercostal arteries, which feed the Artery of Adamkiewicz (supplying the anterior spinal cord).
Surgical intervention carries high risk of paraplegia (Artery of Adamkiewicz damage)
Type B (Descending) Complicated (e.g., malperfusion syndrome, rupture, rapid expansion): Endovascular stenting (TEVAR) or surgery.
Complications
Cardiac Tamponade: Most common cause of death in Type A. c
Acute Aortic Regurgitation: Can lead to acute heart failure/cardiogenic shock.
Organ Ischemia (Malperfusion Syndromes):
Brain: Stroke (carotid artery).
Kidneys: AKI (renal artery).
Gut: Mesenteric ischemia (SMA/IMA).
Spinal cord: Anterior cord syndrome/paraplegia (Artery of Adamkiewicz).