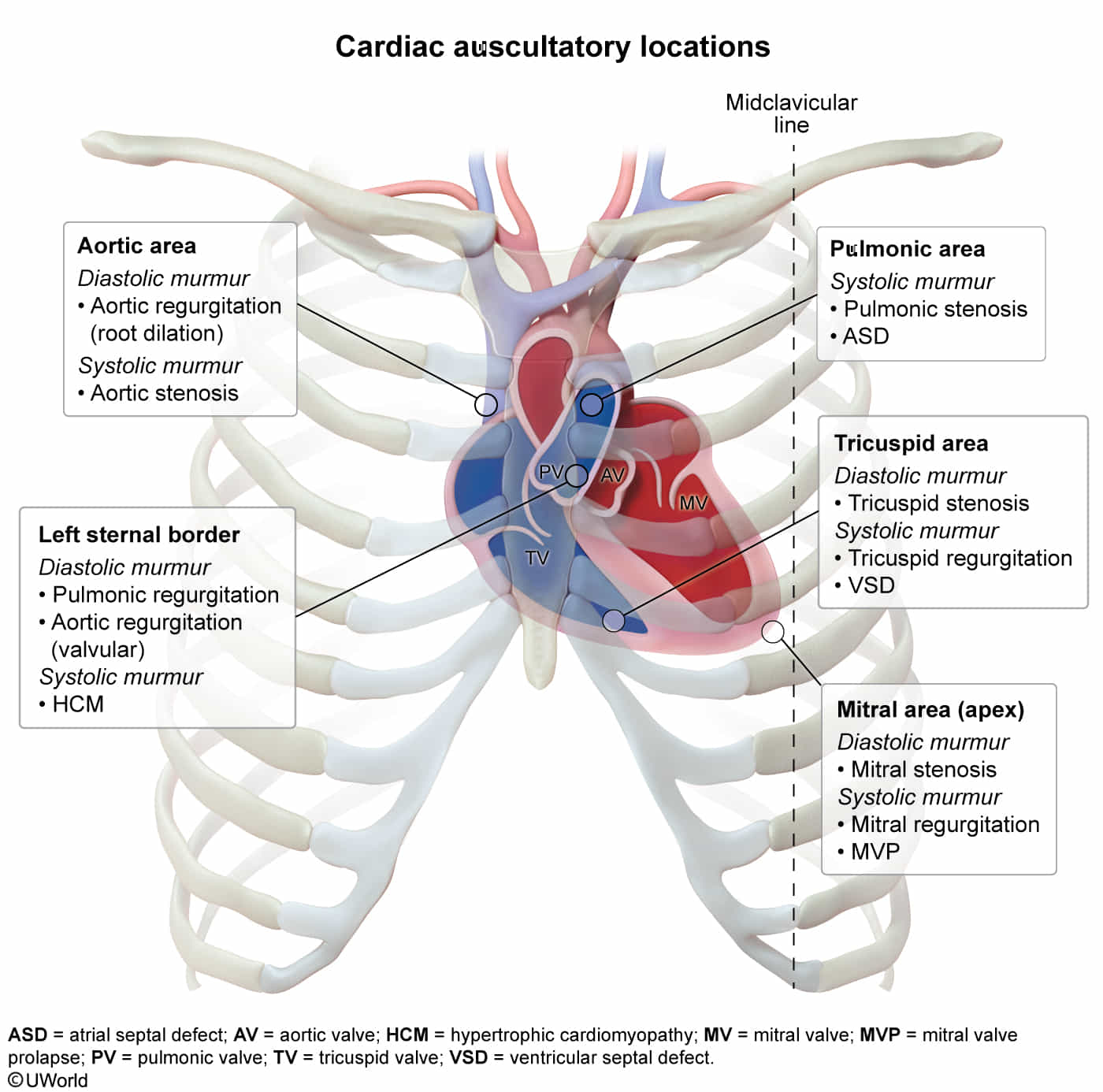
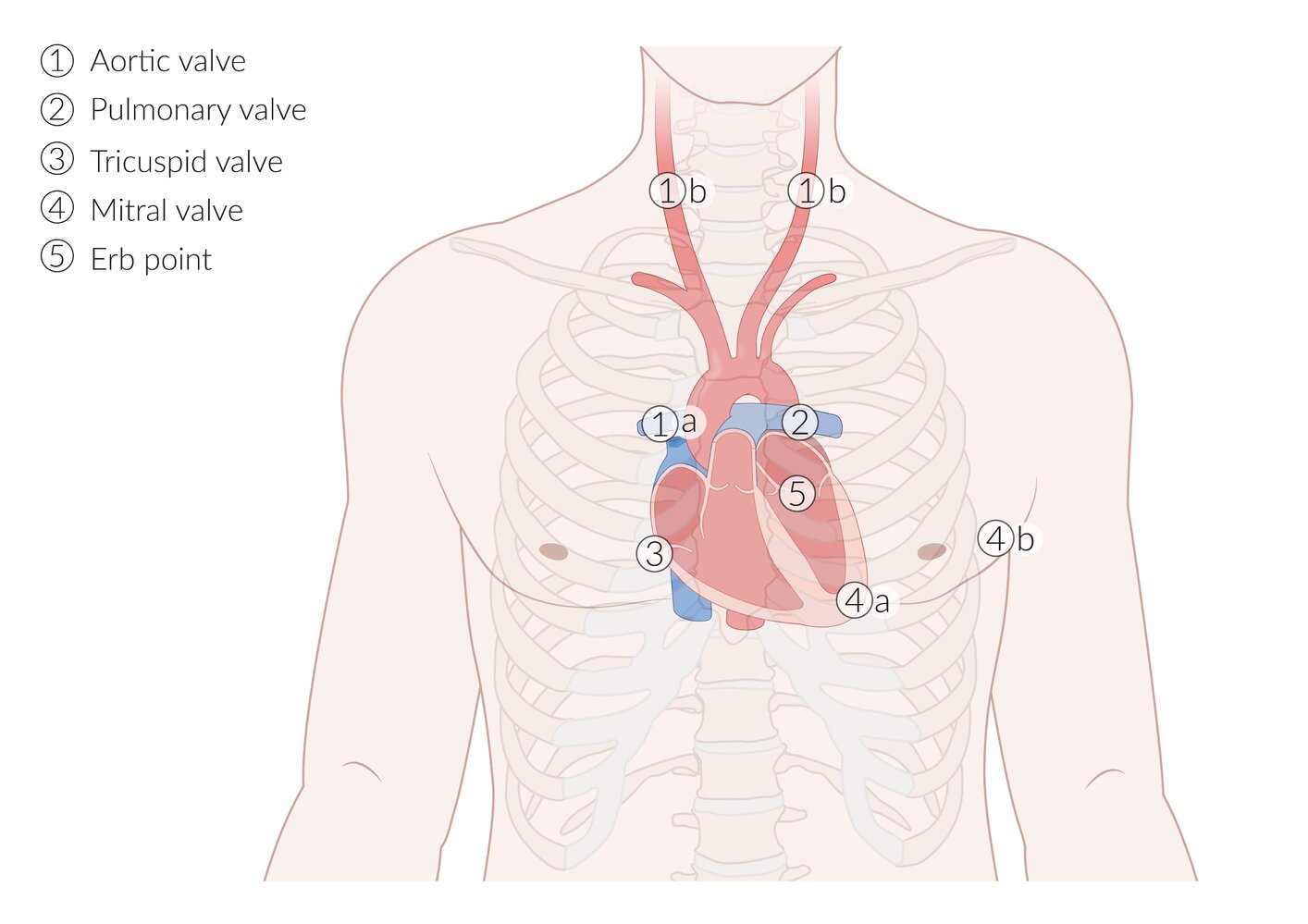
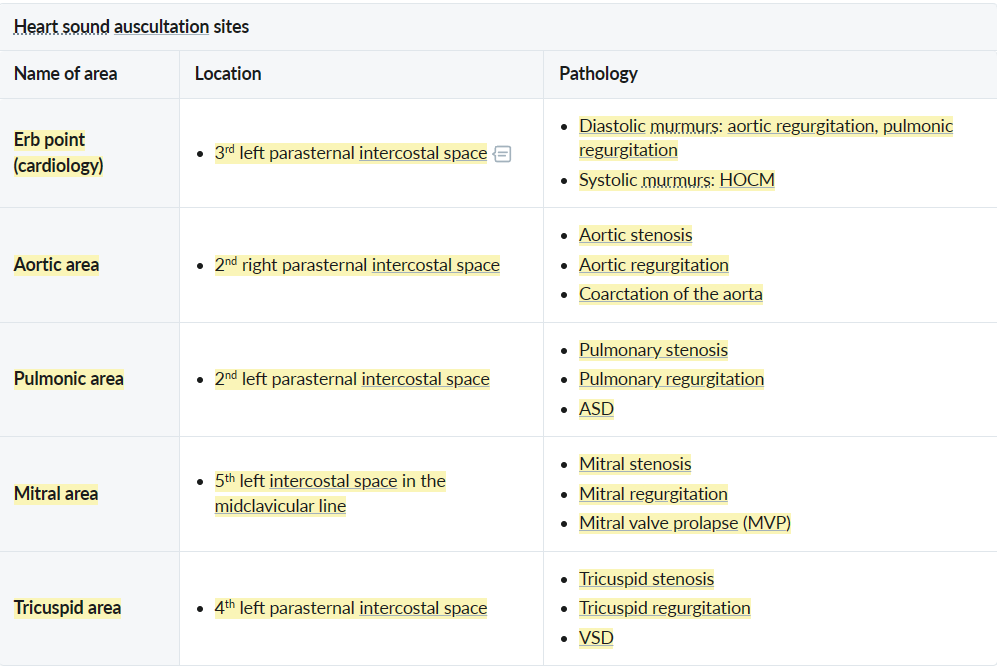
- Right 2nd Intercostal Space (Aortic Area)
- Aortic Stenosis
- Flow Murmur
- Left 2nd Intercostal Space (Pulmonic Area)
- Pulmonic Stenosis
- Atrial Septal Defect (Pulmonary flow murmur)
- Left Sternal Border (3rd-4th Intercostal Space)
- Aortic Regurgitation
- Hypertrophic Cardiomyopathy (HOCM)
- Pulmonic Regurgitation
- Left Lower Sternal Border (Tricuspid Area)
- Tricuspid Regurgitation
- Ventricular Septal Defect (VSD)
- Tricuspid Stenosis
- Apex (Mitral Area)
- Mitral Regurgitation
- Mitral Valve Prolapse
- Mitral Stenosis
- Left Infraclavicular Area
- Patent Ductus Arteriosus (PDA)
Heart murmurs
Benign (Innocent) Murmurs
- Epidemiology & Risk Factors
- Highly prevalent: Occurs in >50% of healthy children & young adults.
- Exacerbated by high-output states: Pregnancy, fever, anemia, hyperthyroidism, exercise, anxiety.
- Clinical Features
- Timing: Early to mid-systolic (never diastolic, holosystolic, or late systolic). c
- Intensity: Grade 2/6 (soft, no palpable thrill). c
- Quality: Musical, vibratory, or blowing (e.g., Still murmur). Not harsh.
- Location: Highly localized (often LLSB or pulmonic area) with no radiation.
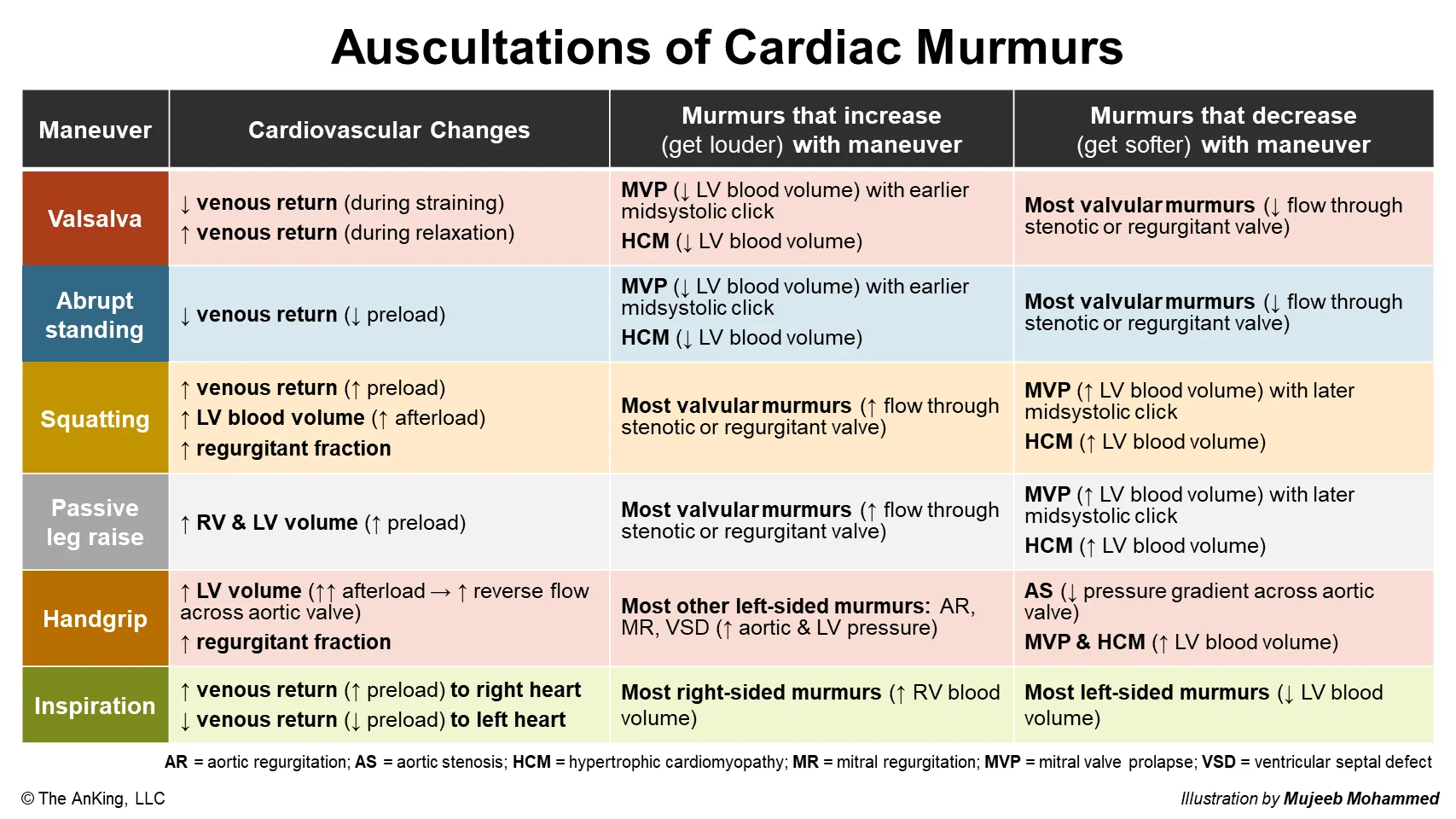
- Dynamic Maneuvers:
- intensity with standing or Valsalva ( venous return).
- intensity with supine position or passive leg raise ( venous return).
- Associated Findings: Normal S1 & S2 (normal physiologic splitting), no extra heart sounds (no clicks, no S3/S4).
- Asymptomatic: No cyanosis, FTT, diaphoresis with feeding, CP, or syncope.
- Common Subtypes:
- Still’s Murmur: LLSB or apex, vibratory/musical (most common in kids). c2
- Louder: Supine position (↑ venous return/preload stretches the ventricle, ↑ stroke volume and ejection velocity).
- Softer: Standing or Valsalva (↓ preload).
- Pulmonary Flow Murmur: LUSB, soft blowing (common in adolescents).
- Cervical Venous Hum: Right supraclavicular, continuous, but easily abolished by neck flexion or jugular compression (exception to the “never continuous” rule).
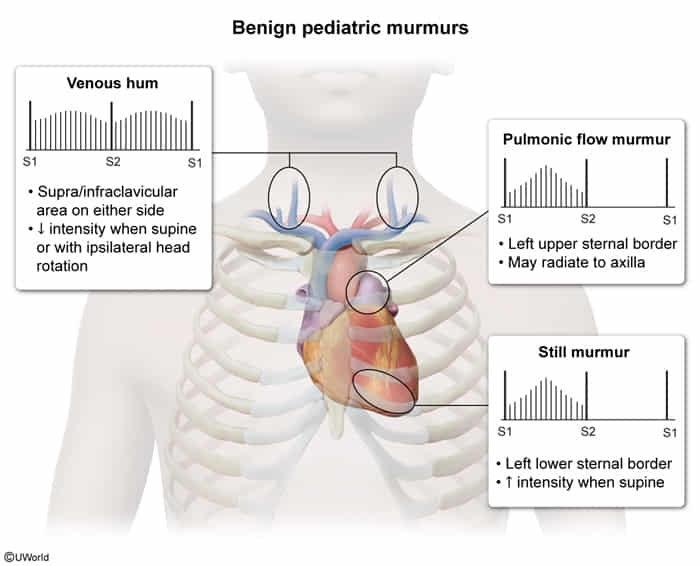
- Still’s Murmur: LLSB or apex, vibratory/musical (most common in kids). c2
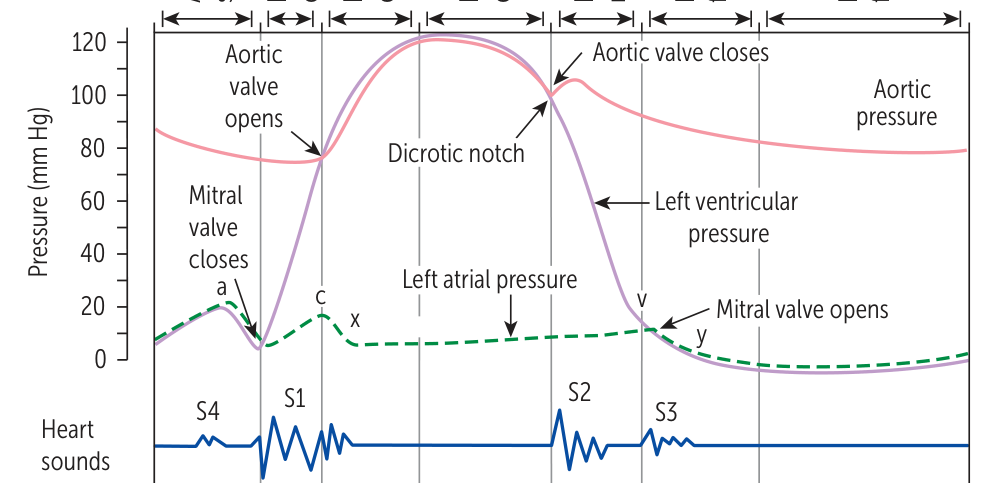
Heart sounds
Extra (gallop) heart sounds
Tip
- S3: volume-overloaded
- Three tree → tree is big and large → ventricle is large
- S4: pressure-overloaded
- Four door → door is hard → ventricle is stiff
Tip
- S3 (Kentucky): sounds like Ken-tuc-ky.
- S4 (Tennessee): sounds like Ten-nes-see, where “Ten” is the S4.
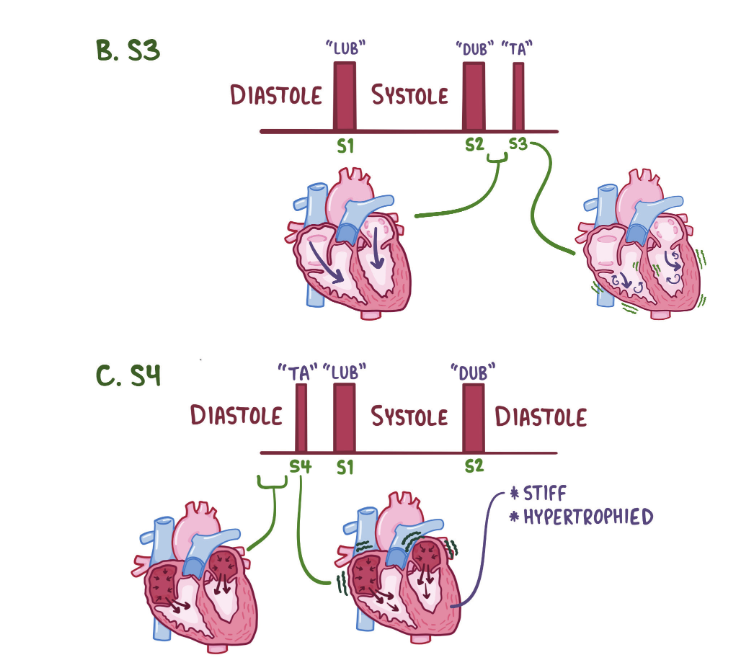
S3
- Features
- Heard just after S2 (after opening of mitral valve)
- Caused by reverberant sound as blood fills an enlarged LV cavity during passive diastolic filling (i.e. end systolic volume is high)
- Associated disorders
- Heart failure with reduced EF
- High-output states (eg, thyrotoxicosis)
- Mitral or aortic regurgitation
- Teens or athletes
- Hearts are trained to handle more blood
S4
- Features
- Heard just before S1 (before closing of mitral valve)
- Caused by blood striking a stiff LV wall during atrial contraction
- As the atria contracts in late diastole against a stiffened ventricle, it must increase its force-production, which creates turbulent blood flow.
- Associated disorders
- Concentric LV hypertrophy
- Restrictive cardiomyopathy
- Acute myocardial infarction
S2 split
Tip
What determines when S2 closes is when the pulmonary artery/aortic pressure can exceed the ventricular pressure.
- Physiological split
- The sound of aortic valve closure (A2) precedes the sound of pulmonary valve closure (P2) during inspiration
- Especially pronounced among young individuals
- Wide split
- Caused by any condition that increases right ventricular afterload or decreases left ventricular preload
- Causes
- Pulmonary hypertension
- Pulmonary valve stenosis
- RBBB
- Fixed split
- Paradoxical split (reversed split)
- Audible during expiration but not inspiration
- Expiration: A2 is heard after P2 during expiration due to delayed closure of the aortic valve (split reversal)
- Inspiration: the closure of the pulmonary valve is also delayed, resulting in A2 and P2 occurring simultaneously (i.e., a paradoxical decrease in the split during inspiration)
- Causes
- Aortic stenosis
- Left bundle branch block
- Audible during expiration but not inspiration
Jugular venous pressure
Cardiovascular examination
- Evaluated using the right internal jugular vein (IJV) with pt at 45-degree angle.
- Normal JVP: < 8 cm H2O (measured as vertical distance from sternal angle + 5 cm). c
- ↑ JVP indicates elevated right-sided heart pressures or mechanical obstruction of venous return.
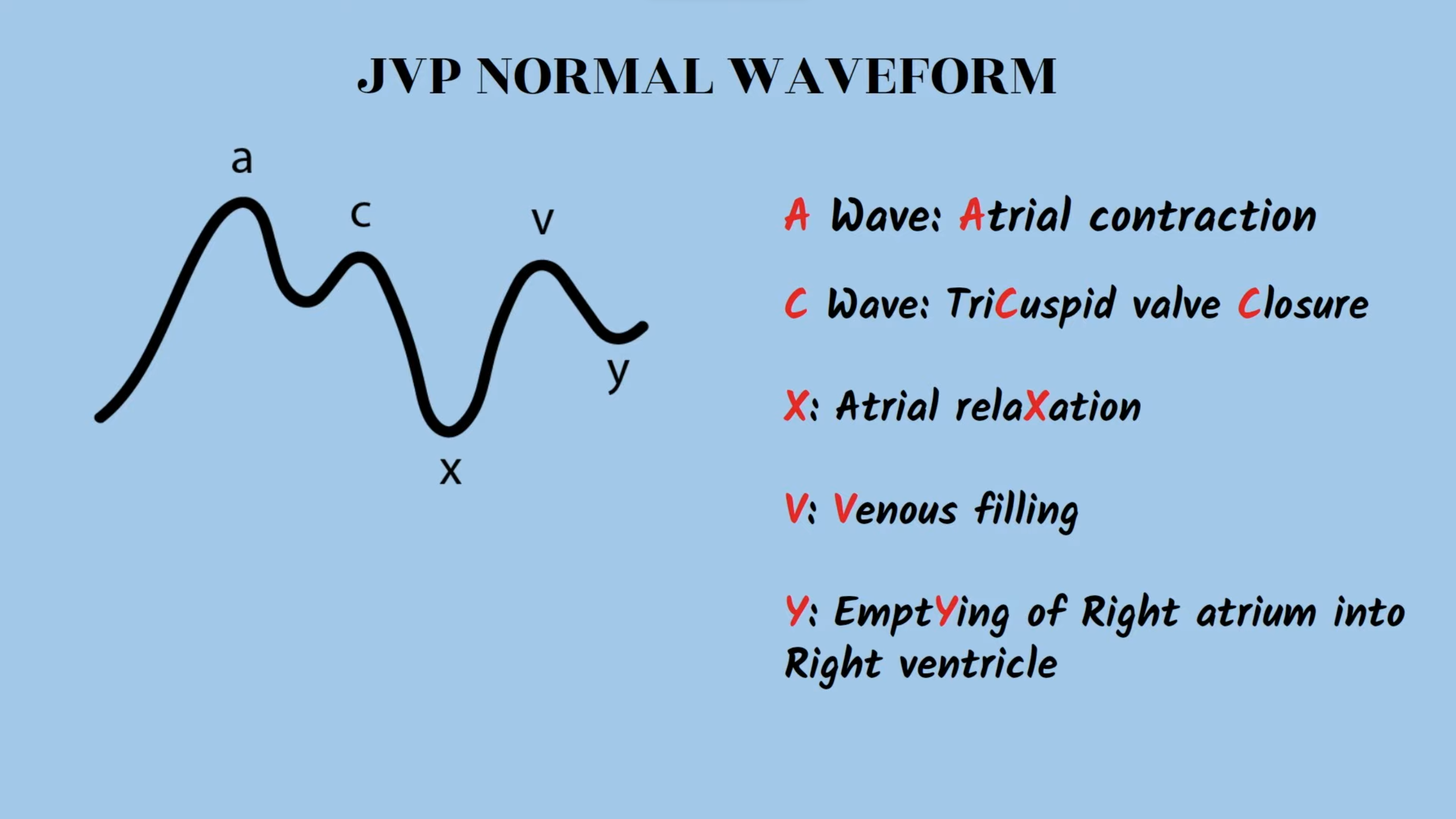
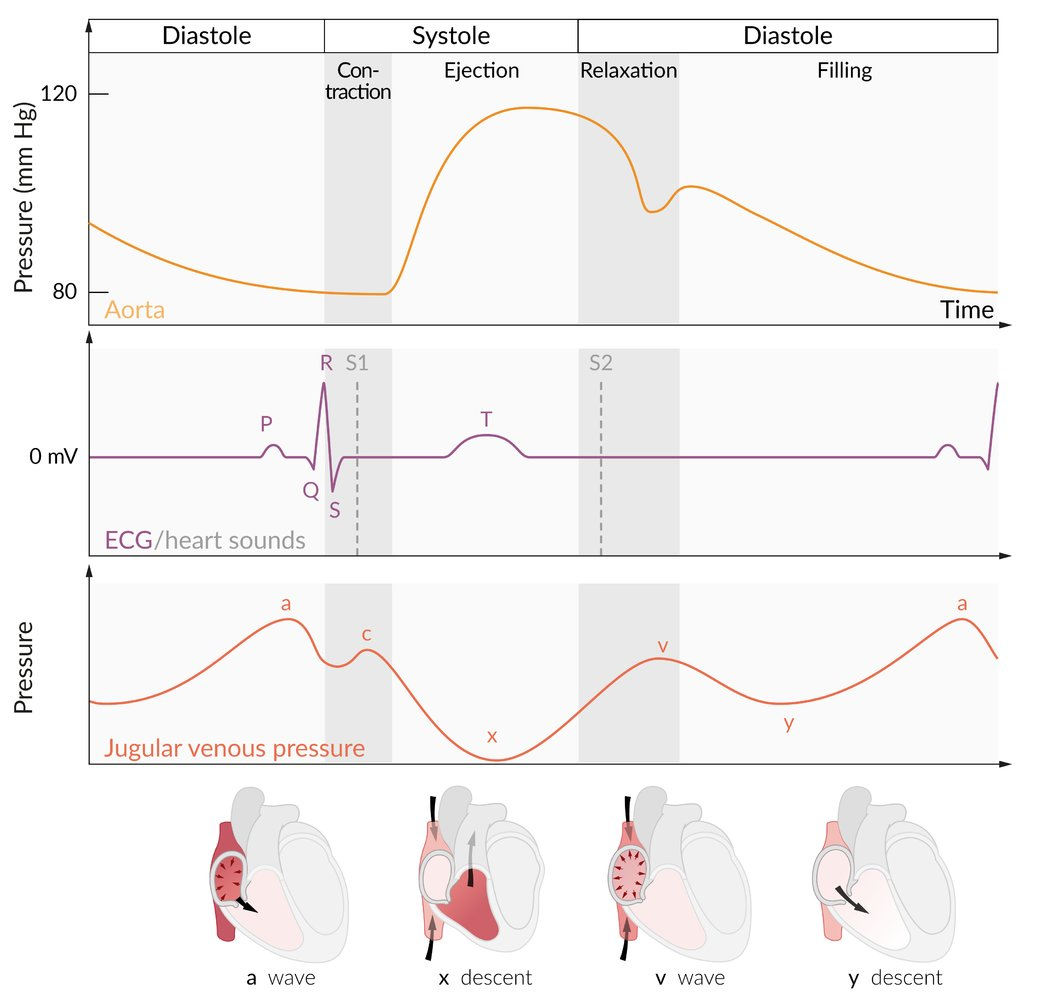
Normal Waveform Components
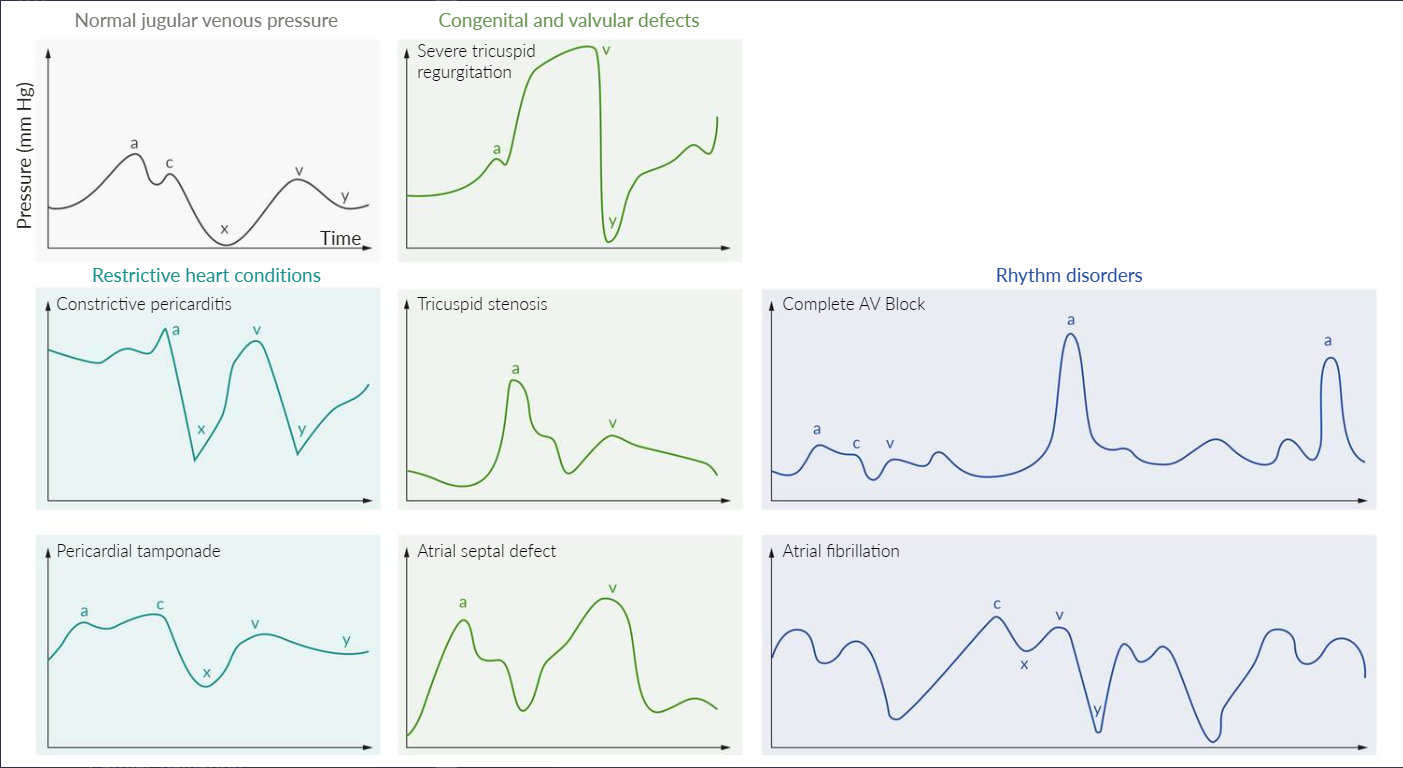
Abnormal JVP Waveforms
- Large ‘a’ wave: Increased resistance to right atrial emptying.
- Causes: Tricuspid stenosis, right ventricular hypertrophy, pulmonary hypertension.
- Cannon ‘a’ waves: Very large, intermittent ‘a’ waves.
- Pathophysiology: Right atrium contracts against a closed tricuspid valve (AV dissociation).
- Causes: Complete heart block (third-degree), ventricular tachycardia, premature ventricular/junctional contractions.
- Absent ‘a’ wave: No coordinated atrial contraction.
- Cause: Atrial fibrillation.
- Large ‘v’ wave (or c-v fusion wave):
- Pathophysiology: Blood regurgitates into the right atrium during ventricular systole.
- Cause: Tricuspid regurgitation.
- Rapid/Steep ‘y’ descent (Friedreich’s sign):
- Pathophysiology: Rapid, early diastolic filling of a stiff or non-compliant ventricle.
- Causes: Constrictive pericarditis, restrictive cardiomyopathy.
- Slow ‘y’ descent:
- Pathophysiology: Obstruction of right ventricular filling.
- Causes: Tricuspid stenosis, right atrial myxoma.
- Blunted/Absent ‘y’ descent:
- Pathophysiology: Impaired right ventricular filling due to external pressure.
- Cause: Cardiac tamponade.
Pathology
Common abnormalities of the JVP waveform include:
Link to original
- Constrictive pericarditis: elevated JVP (due to increased external atrial pressure) with a prominent x (exaggerated atrial relaxation) and y (early rapid ventricular filling) descent
- Cardiac tamponade: elevated JVP (due to increased external atrial pressure), a prominent x descent (exaggerated atrial relaxation), and a blunt or absent y descent (minimal ventricular filling)
- Tricuspid regurgitation: prominent v wave as the blood from the right ventricle regurgitates into the right atrium during ventricular systole (atrial diastole), increasing interatrial pressure and volume
- Tricuspid stenosis: giant a wave due to high right atrial systolic pressure
- Atrial septal defect: v wave ≥ a wave due to the left-to-right shunting of blood
- Third-degree atrioventricular (AV) block: cannon a waves due to the loss of AV synchronization and contraction of the atria against a closed tricuspid valve
- Atrial fibrillation: absent a waves due to ineffective contraction of the atria