| Stone | Radio-density | Urine pH | Crystal Shape | Key Association |
|---|---|---|---|---|
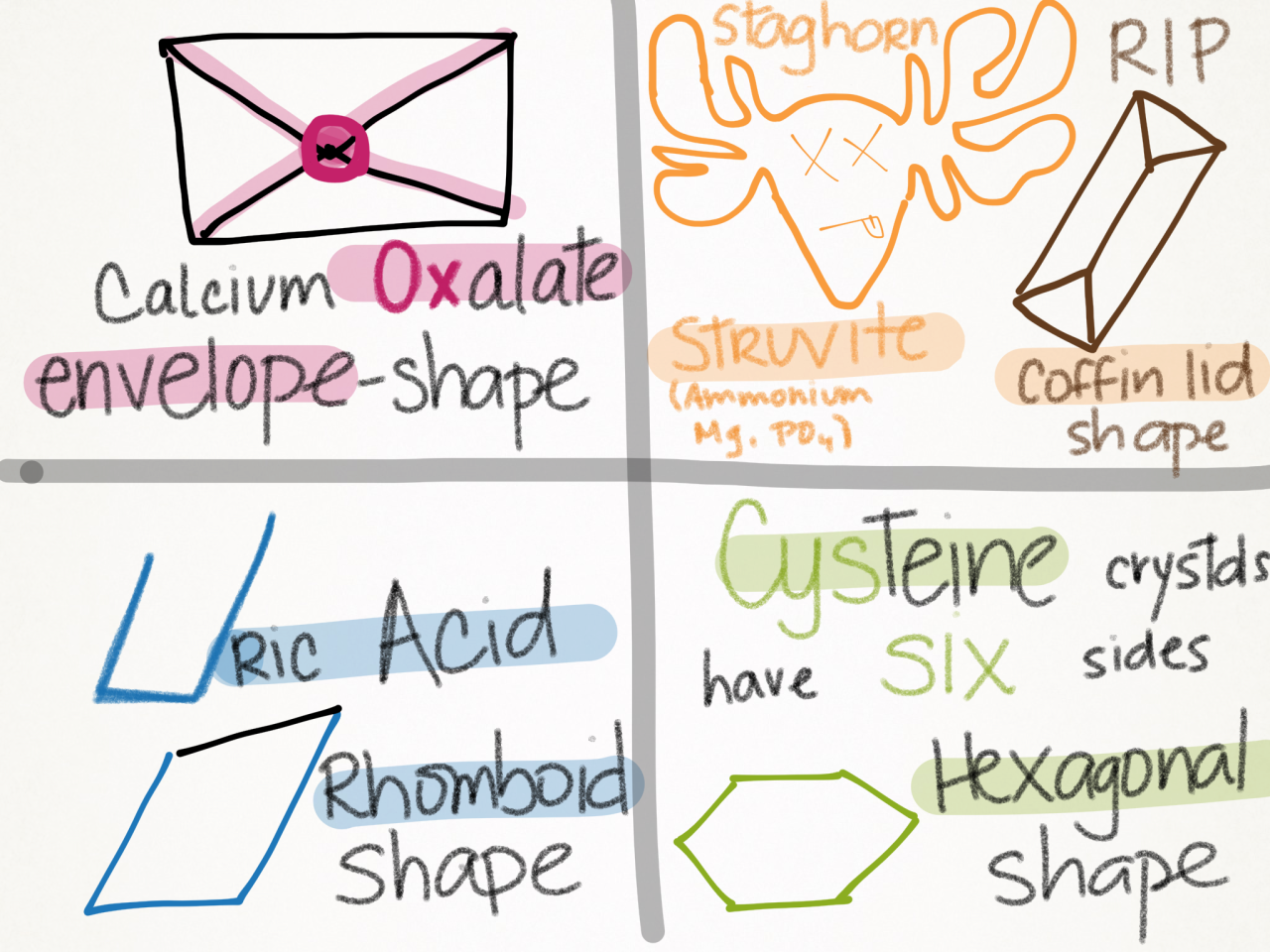
| Calcium Oxalate | Opaque | ↓ | Envelope | Most common; Idiopathic hypercalciuria |
| Calcium Phosphate | Opaque | ↑ | Wedge-shaped | Distal RTA Type 1 |
| Uric Acid | Lucent | ↓ | Rhomboid | Gout; high cell turnover |
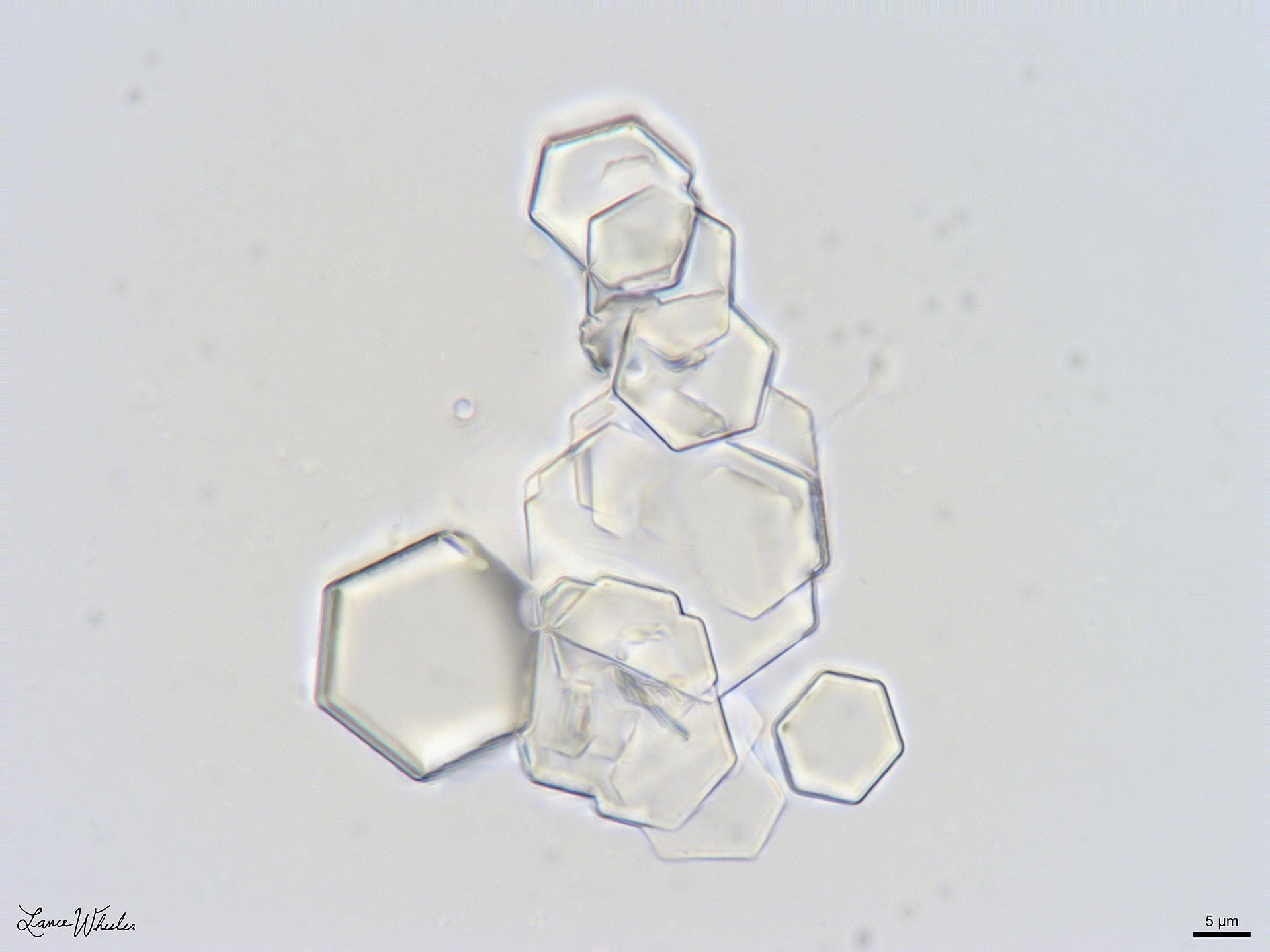
| Cystine | Faintly Opaque | ↓ | Hexagonal | Genetic (COLA transporter defect) |
| Struvite (MAP) | Opaque | ↑ | Coffin Lid | Urease+ microbes (Proteus); Staghorn |
Classifications
Mnemonic
PH
- Acidic Urine (↓ pH < 5.5)
- Calcium Oxalate: Oxalate is less soluble in acidic urine → precipitation favored
- Uric Acid: Uric acid (protonated form) is insoluble at low pH; urate (deprotonated) is soluble at higher pH → stones form when urine is acidic
- Cystine: Cystine solubility ↓ dramatically at pH < 7; becomes insoluble in acidic conditions
- Alkaline Urine (↑ pH > 7)
- Calcium Phosphate: Phosphate salts (PO₄³⁻) are less soluble in alkaline conditions → precipitation occurs; associated with Type 1 RTA (inability to acidify urine)
- Struvite (Magnesium Ammonium Phosphate): Urease-producing bacteria (Proteus, Klebsiella) split urea → releases ammonia (NH₃) → ↑ urine pH to 7-8 → creates alkaline environment where struvite crystallizes
Calcium stones
Calcium oxalate stones
Etiology
- Most common nephrolithiasis type (~75-80% of all cases).
- Dehydration: Low urine volume increases solute concentration.
- Idiopathic hypercalciuria: Normocalcemic, hypercalciuric (most common metabolic abnormality).
- Hyperoxaluria:
- Dietary: Excess consumption of spinach, rhubarb, nuts, tea, cocoa.
- Enteric: Malabsorption (e.g., Crohn’s disease, gastric bypass, celiac disease) -> unabsorbed fat binds Ca -> free oxalate absorbed in colon.
- Vitamin C > Vitamin C toxicity: Metabolized directly into oxalate.
- Ethylene glycol toxicity c
- Hypocitraturia: Citrate binds Ca to form soluble complexes. Low citrate (e.g., Type 1 RTA, chronic diarrhea) increases free Ca.
- Diet: High sodium (promotes calciuria), high animal protein, low dietary calcium (increases GI absorption of oxalate).
Tip
Individuals with higher (but not excessive) calcium intake paradoxically have a lower risk of calcium oxalate stone formation. Dietary calcium binds oxalate in the gut to form insoluble calcium oxalate, which is eliminated in the feces. This reduces the amount of oxalate absorbed into the body and excreted in the urine, reducing stone formation.
Diagnosis
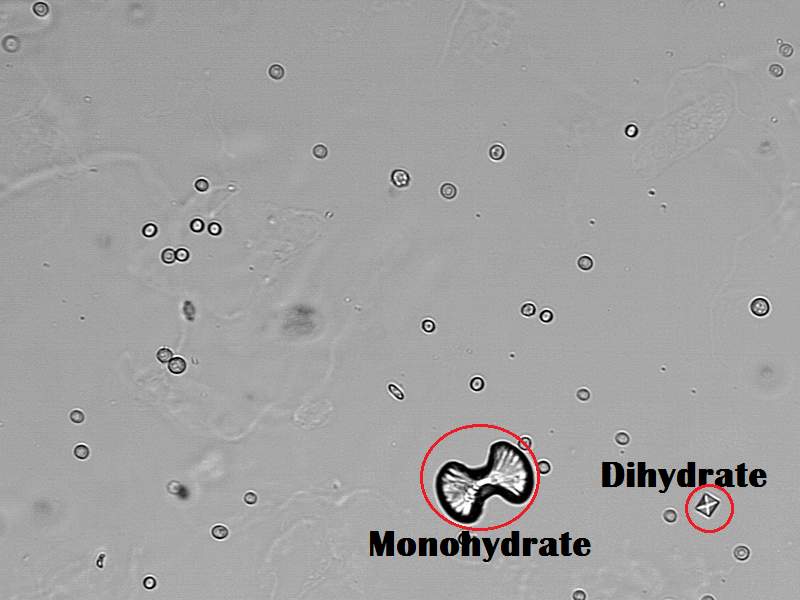
- Urine microscopy: dumbbell-shaped or octahedron-shaped crystals
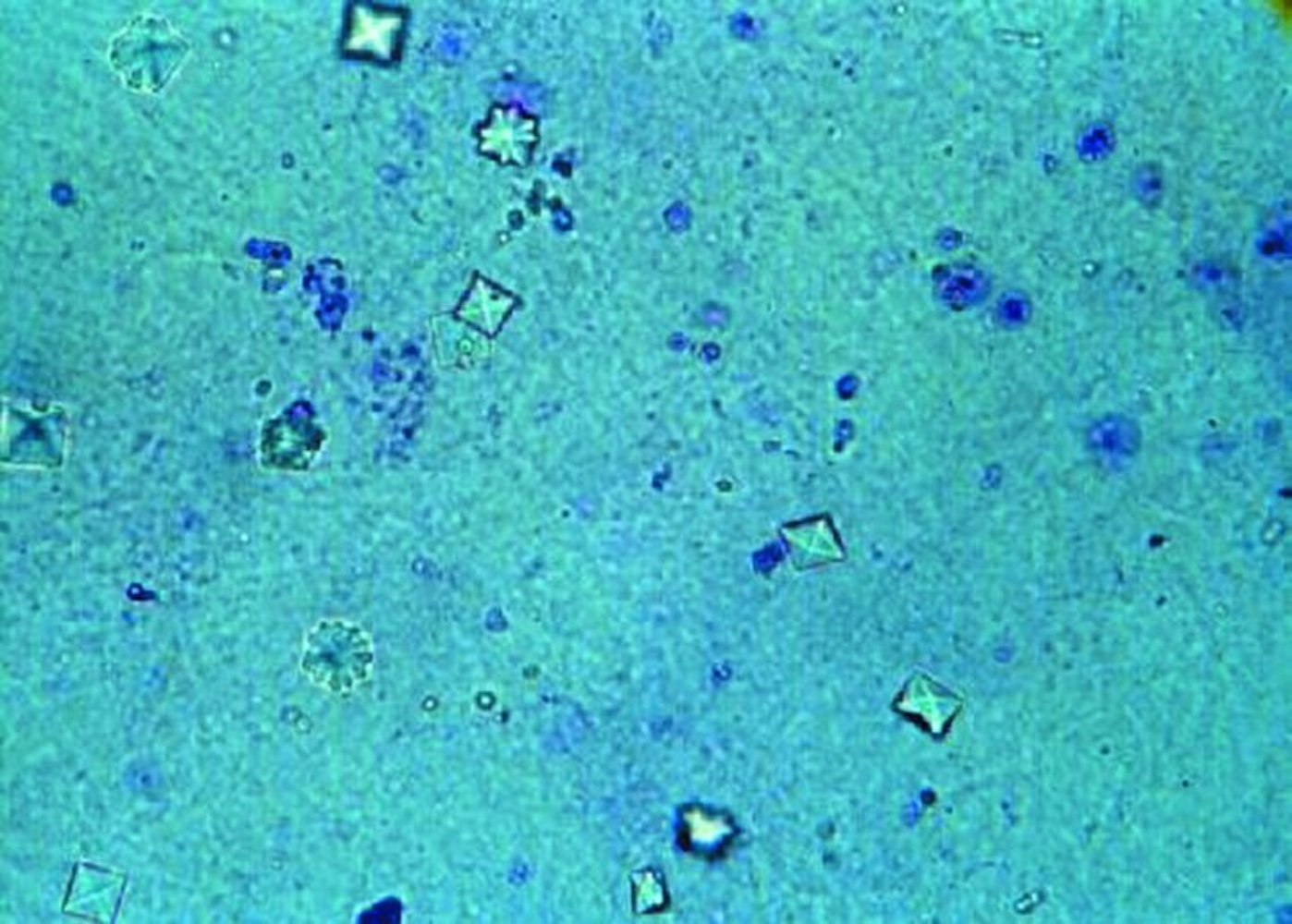
- The monohydrate calcium oxalate crystal is described as the “picket fence” form. These dumbbells shaped crystals are common in ethylene glycol toxicity. The dihydrate form is octahedral or “envelope” shaped.
- The monohydrate calcium oxalate crystal is described as the “picket fence” form. These dumbbells shaped crystals are common in ethylene glycol toxicity. The dihydrate form is octahedral or “envelope” shaped.
- X-ray (or CT): radiopaque stones
Tip
Serum calcium can be normal or elevated.
Treatment
- Hydration
- Dietary modification
- Low sodium, low animal protein (Low sodium enhances renal tubular reabsorption of sodium and calcium, decreasing urinary calcium levels. Animal protein consumption increases calcium excretion in urine.) c
- Reduced intake of oxalate-rich foods and supplemental vitamin C
- Calcium intake should not be restricted (restriction increases risk of hyperoxaluria, and thereby, the risk for osteoporosis)
- Thiazide diuretics for recurrent calcium-containing stones with idiopathic hypercalciuria (i.e., no hypercalcemia)
- Urine alkalinization (e.g., with potassium citrate)
- Possibly citrate supplementation
Calcium phosphate stones
Etiology
- Hyperparathyroidism (brushite)
- Type 1 renal tubular acidosis (brushite)
- Develop in persistently alkalic urine
Diagnosis
- Urine microscopy: wedge-shaped crystals

- X-ray (or CT): radiopaque stones
Prevention
- Hydration
- Thiazide diuretics
- Diet low in sodium
Uric acid stones
Etiology
- Hyperuricemia and hyperuricosuria
- Gout
- High cell turnover (e.g., tumor lysis syndrome, myelodysplastic syndrome)
- Diabetes mellitus, metabolic syndrome
- Chronic diarrhea
Diagnosis
- Urine microscopy: rhomboid/needle-shaped crystals
- X-ray: radiolucent stones
- CT: can be visible but are usually only minimally visible (not as visible as calcium stones)
Treatment
- Hydration
- Oral chemolitholysis (e.g., potassium citrate) via urine alkalinization
- Uric acid (pKa = 5.4) is soluble at physiologic pH, but precipitates in an acidic environment. The lowest pH along the nephron is found in the distal tubules and collecting ducts; so these are the segments of the nephron that become obstructed by uric acid crystals. Obstructive uropathy and acute renal failure follow.
- Uric acid stones are unique in that they can usually be dissolved by alkalizing the urine. In other stones, urine alkalinization is used for prophylaxis rather than treatment.
- Low-purine diet
- Allopurinol
Mnemonic
Uric acid stones are radiolUcent (x-ray negative).
Warning
Uricosuric agents (e.g., probenecid) increase the excretion of uric acid, which can accelerate the formation of stones.
Cystine stones
Etiology
- Autosomal recessive defect in cystine-reabsorbing PCT transporter → impaired proximal renal tubular absorption of dibasic amino acids → Cystinuria → cystine stone formation (as cystine is poorly soluble)
- Develop in persistently acidic urine
Clinical features
Recurrent kidney stones (manifesting with e.g., flank pain) starting in childhood
Diagnosis
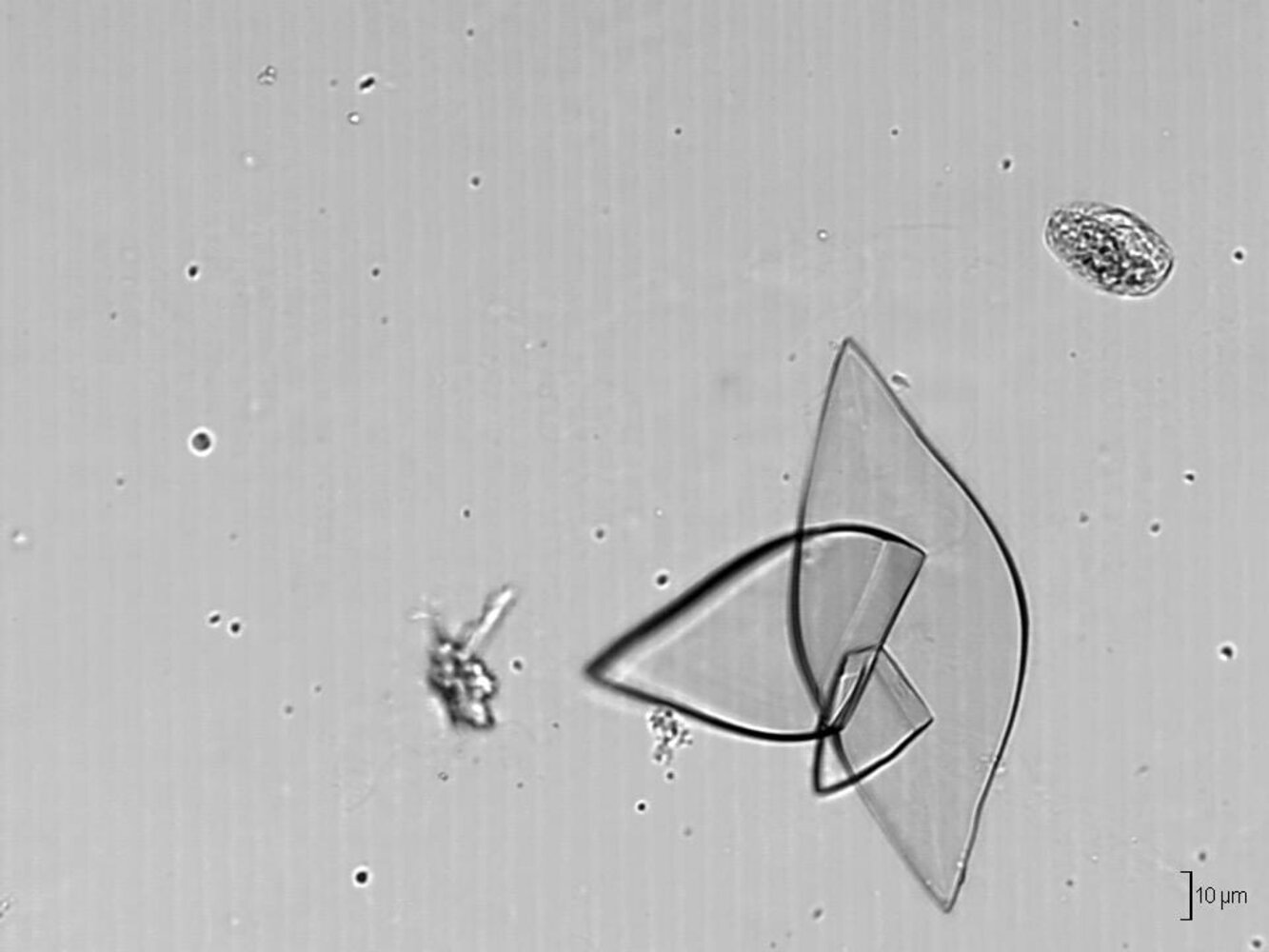
- Urine microscopy: hexagonal crystals
- X-ray (or CT)
- Weakly radiopaque stones
- Possibly staghorn calculi
- Positive cyanide nitroprusside test
Struvite stones (magnesium ammonium phosphate stones)
Etiology
- Upper UTI with urease-producing bacteria such as Proteus mirabilis (most common), Klebsiella pneumoniae
- E. coli is urease-negative and does not cause struvite stones.
- These bacteria convert urea to ammonia → elevated ammonia causing alkaline urine → precipitation of the ammonium magnesium phosphate salt → crystal and stone formation
- Urea → 2 NH3 + CO2
- NH3 + H2O → NH4+ + OH−
- Grow rapidly into a branched staghorn calculus that fills the renal calyces and pelvis.
- Over time, the affected kidney can atrophy due to recurrent infection and chronic obstructive nephropathy.
Treatment
- Antibiotic treatment of urinary tract infections
- Hydration
- Urine acidification
- Usually require surgical stone removal
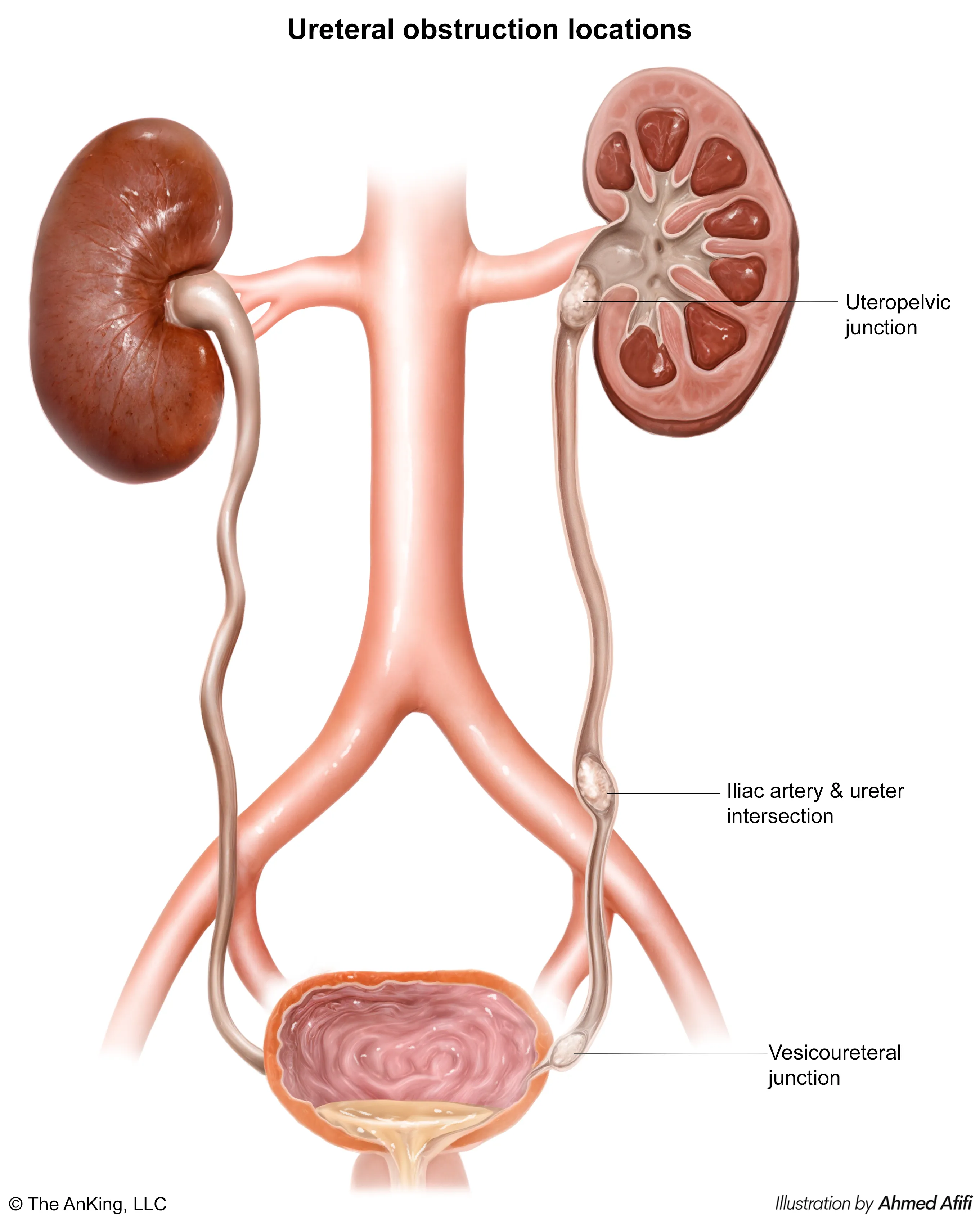
Pathophysiology
There are three main physiological constrictions of the ureter where stones often lodge:
- Ureteropelvic junction (UPJ)
- Crossing of the iliac vessels at the pelvic brim
- Ureterovesical junction (UVJ)
- Filtration Mechanics: Obstruction → ↑ Tubular pressure → ↑ Hydrostatic pressure in Bowman space → ↓ GFR.
- Hemodynamics:
- Acute: Afferent dilation (PGE2) to maintain flow.
- Chronic: Afferent vasoconstriction (Angiotensin II, Thromboxane A2) → Ischemia & Hydronephrosis.
- Tubular Dysfunction: High pressure damages tubular epithelium and downregulates transport channels. t
- Concentrating Defect: Downregulation of Aquaporins → ADH resistance (Nephrogenic Diabetes Insipidus).
- Acidification Defect: Impaired / secretion → Type 4 RTA (Hyperkalemia).
- Post-Obstructive Diuresis: Massive polyuria after relief due to osmotic load (urea) and transient tubular incompetence.
Clinical features
- Fluctuating urine output (alternating polyuria and oliguria). c
Diagnostics
Treatment
- Acute Management:
- Analgesia: NSAIDs (e.g., IV Ketorolac) are first-line (superior to opioids because they decrease ureteral spasm). Opioids (e.g., Morphine) used for refractory pain.
- Hydration: Aggressive IVF only if Pt is dehydrated; routine overhydration does not facilitate stone passage and can worsen pain.
- Antiemetics: IV Metoclopramide or Ondansetron.
- Surgical & Expulsive Stratification by Stone Size:
- Stones < 5 mm: Spontaneous passage in > 80%. Managed conservatively with home hydration, strain urine to catch stone, and oral analgesics.
- Stones 5-10 mm: Medical expulsive therapy with Tamsulosin (alpha-1 blocker to relax distal ureteral smooth muscle). Follow closely. c
- Stones > 10 mm: Unlikely to pass spontaneously. Require intervention:
- Proximal ureteral/renal stones < 2 cm: Extracorporeal Shockwave Lithotripsy (ESWL) or Ureteroscopy (URS).
- Distal ureteral stones: Ureteroscopy (URS) with basket extraction.
- Very large stones (> 2 cm, e.g., staghorn): Percutaneous Nephrolithotomy (PCNL).
- Urologic Emergency Indicators:
- Signs of concomitant infection (fever, chills, pyuria) + obstruction (hydronephrosis, AKI, anuria).
- Management: Emergency decompression via retrograde ureteral stent placement or percutaneous nephrostomy. Do not perform lithotripsy in an infected, obstructed system.
- Long-term Prevention:
- General: Increase fluid intake (> 2.5 L/day), restrict sodium and animal protein.
- Calcium Stones: Do NOT restrict dietary calcium (decreased calcium increases gut absorption of free oxalate). Give Thiazide diuretics (increases renal Ca reabsorption) and Potassium Citrate (citrate binds calcium in urine, preventing precipitation).
- Uric Acid & Cystine Stones: Alkalinize urine with Potassium Citrate/Bicarbonate. Add Allopurinol for refractory uric acid stones. Penicillamine or Tiopronin for refractory cystine stones. c
- Potassium citrate is metabolized in the liver to bicarbonate (), which is excreted in the urine.
Special patient groups
Nephrolithiasis in children
- Epidemiology & Risk Factors:
- Metabolic anomalies (>75%): Hypercalciuria (most common), hypocitraturia (loss of crystallization inhibitor), cystinuria.
- Meds/Diet: Ketogenic diet, topiramate (carbonic anhydrase inhibitor → hypocitraturia/hypercalciuria), high Na, low fluid intake.
- Infection: Urease(+) pathogens (Proteus, Klebsiella) → struvite/triple phosphate stones (coffin-lid crystals).
- Clinical Features:
- Infants: Painless hematuria, poor feeding, vomiting, colic.
- Older kids: Acute flank pain radiating to groin (renal colic), dysuria, hematuria (~90%).
- Diagnosis:
- Initial: Renal & bladder US (first-line, avoids radiation, detects hydronephrosis).
- Gold Standard: Non-contrast low-dose CT abd/pelvis (if US equivocal).
- Crystals: Hexagonal (cystine), coffin-lid (struvite), envelope (Ca oxalate).
- Workup: 24-hr urine collection (fluid volume, Ca, oxalate, citrate, cystine) post-acute phase.
- Differential Diagnostics:
- Appendicitis: RLQ pain, fever, leukocytosis; no hematuria.
- UTI/Pyelonephritis: Pyuria, bacteriuria, fever; no acute colic.
- Torsion (Testicular/Ovarian): Acute scrotal/pelvis pain, abnormal Doppler flow.
- Management:
- Acute:
- IVF (1.5–2x maintenance) + pain control with NSAIDs (first-line).
- Tamsulosin (alpha-blocker) to aid passage of stones < 10 mm.
- Surgical: ESWL/URS (stones ≤ 20 mm) or PCNL (> 20 mm/staghorn).
- Urgent decompression (stent/nephrostomy) if obstruction + infection (urosepsis).
- Prevention: High fluids, low Na.
- Ca stones: Thiazides (↓ urinary Ca) + potassium citrate (alkalinizes urine).
- Cystine: Alkalinization (pH > 7.5), thiol-binding agents (tiopronin).
- Acute:
- Complications:
- Urosepsis (obstructed UTI).
- Hydronephrosis & post-renal AKI.
- CKD/renal scarring.