↓ Production of urine → ↑ extracellular fluid volume → total-body volume overload
↓ Excretion of waste products (e.g., urea, drugs)
↓ Excretion of phosphate → hyperphosphatemia
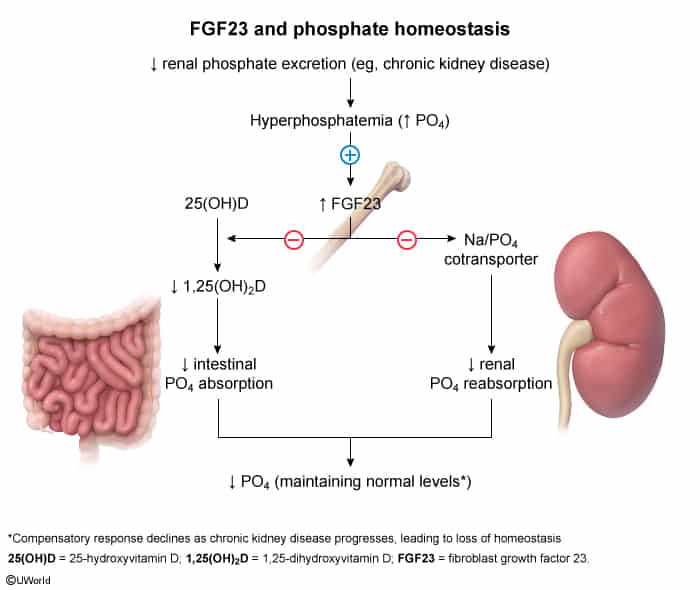
During the early stages of CKD, plasma phosphate levels will typically be normal due to the increased secretion of fibroblast growth factor 23 (FGF23).
FGF23 is produced by osteoblasts in response to initial hyperphosphatemia and increased calcitriol.
Increased secretion of FGF23 leads to increased phosphate secretion and suppressed conversion of 25-hydroxyvitamin D to 1,25-dihydroxyvitamin D.
In advanced CKD, the effects of FGF 23 subside (most likely due to development of resistance in target tissues).
↓ Maintenance of acid-base balance → metabolic acidosis
↓ Hydroxylation of calcifediol → ↓ production of calcitriol → (in combination with ↓ excretion of phosphate) → ↓ serum Ca2+ → ↑ PTH
↓ Erythropoietin → ↓ stimulation of erythropoiesis
Clinical features
Manifestations of uremia
Definition: Uremia is defined as the accumulation of toxic substances due to decreased renal excretion. These toxic substances are mostly metabolites of proteins such as urea, creatinine, β2 microglobulin, and parathyroid hormone.
Uremic fetor: characteristic ammonia- or urine-like breath odor
Dermatological manifestations
Pruritus
Accumulation of histamine
Skin color changes (e.g., hyperpigmentation, pallor due to anemia)
Uremic frost: uremia leads to high levels of urea secreted in the sweat, the evaporation of which may result in tiny crystallized yellow-white urea deposits on the skin.
Serositis
Uremic pericarditis: a complication of chronic kidney disease that causes fibrinous pericarditis
Clinical features: chest pain worsened by inhalation
Physical examination findings
Friction rub on auscultation
ECG changes normally seen in nonuremic pericarditis (e.g., diffuse ST-segment elevation) are not usually seen.
Pleuritis
Neurological symptoms
Asterixis
Signs of uremic encephalopathy
Seizures
Somnolence
Coma
Peripheral neuropathy → paresthesias
Hematologic symptoms
Anemia
Leukocyte dysfunction → ↑ risk of infection
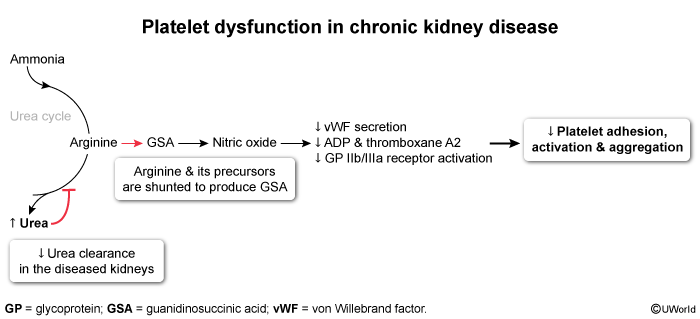
↑ Bleeding tendency caused by abnormal platelet adhesion and aggregationc
Urinalysis: Proteinuria is a key marker of progression. Waxy casts may be seen in advanced disease.
Imaging: Ultrasound to assess kidney size (typically small/echogenic in CKD, except in PCKD/diabetic nephropathy).
Treatment
Delay Progression:
Tight glycemic control (HbA1c < 7.0%).
Tight BP control (< 130/80 mmHg).
ACEi or ARB: First-line for HTN in pts with albuminuria (UACR ≥\ge≥ 30 mg/g) to reduce intraglomerular pressure.
SGLT2 inhibitors (e.g., empagliflozin): Highly high-yield; proven to slow CKD progression and reduce CV mortality in both diabetic and non-diabetic CKD.
Avoid nephrotoxins: Strict avoidance of NSAIDs, IV contrast (unless clinically vital), aminoglycosides.
Dietary Modifications:
Sodium restriction (< 2 g/day), potassium restriction, and phosphorus restriction.
Moderate protein restriction (0.8 g/kg/day in non-dialysis pts).
Complication Management:
Anemia of CKD: Give ESA (Erythropoiesis-stimulating agents) like epoetin alfa. Crucial: Must check and replete iron stores before starting ESA. Target Hb is 10–11.5 g/dL (higher targets increase stroke and CV risk).
Mineral and Bone Disorder:
Phosphate binders (e.g., sevelamer, calcium acetate) taken with meals.
Active vitamin D (calcitriol) or calcimimetics (cinacalcet) to suppress high PTH.
Fluid Overload: Loop diuretics (e.g., furosemide). Note that thiazides are ineffective if GFR < 30.
Uremic Bleeding: Give DDAVP (desmopressin) prior to procedures (increases release of vWF/Factor VIII from endothelial stores to temporarily correct platelet dysfunction).
Modalities: Hemodialysis, Peritoneal Dialysis, or Renal Transplantation (treatment of choice; associated with the lowest long-term mortality).
Complications
Anemia of chronic kidney disease
Pathophysiology: ↓ synthesis of erythropoietin → ↓ stimulation of RBC production → normocytic, normochromic anemia
Management
Consider erythropoietin-stimulating agents (ESAs): for patients with Hb < 10.0 g/dL
Adverse effects: ↑ risk of thromboembolism; ↑ risk of hypertension
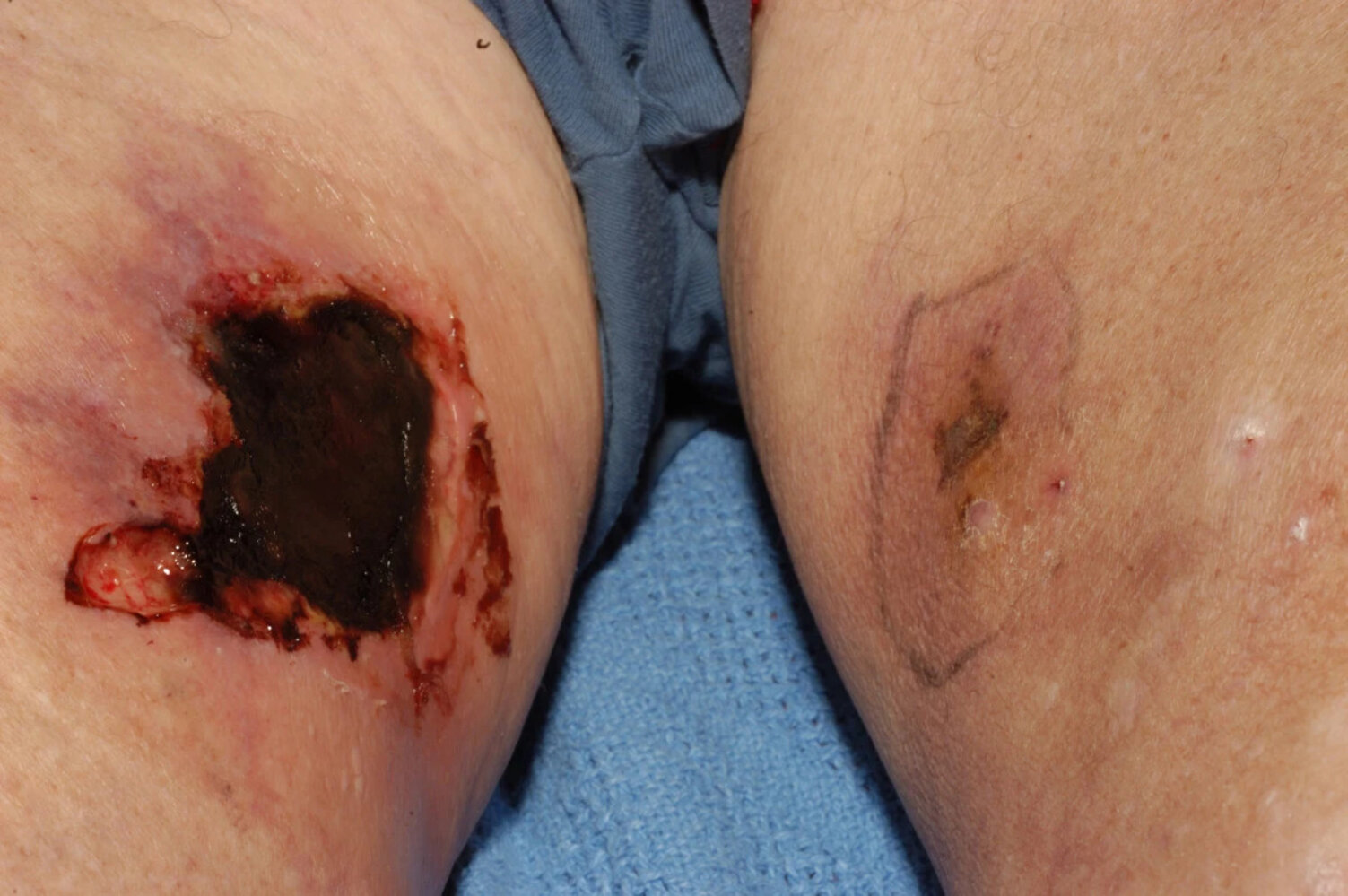
Calciphylaxis (Calcific Uremic Arteriolopathy)
Definition: a rare but potentially life-threatening condition characterized by dermal and subcutaneous arteriolar calcifications that cause painful skin necrosis
high calcium × phosphorus product with mineral deposition in vascular walls c
Risk Factors: ESRD (esp. pts on dialysis), warfarin use (inhibits calcification inhibitor Gla protein), obesity, DM, hyperparathyroidism.
Clinical Features: Severe pain, violaceous, indurated plaques/nodules progressing to necrotic ulcers with black eschar on adipose-rich areas (thighs, abdomen).
Diagnosis:
Initial: Clinical presentation.
Confirmatory/Gold Standard: Deep punch biopsy (shows medial calcification of small/medium arterioles & thrombosis). c