Epidemiology
Etiology
Potassium excess: due to altered K+ metabolism or intake
Reduced excretion: acute and chronic kidney disease
Endocrine causes: hypocortisolism, hypoaldosteronism
Drugs: potassium-sparing diuretics , ACE inhibitors, angiotensin receptor blockers, NSAIDs , and trimethoprim-sulfamethoxazole c
Especially in HIV patients who are taking high-dose TMP-SMX Similar to the actions of amiloride, trimethoprim blocks the epithelial sodium channel in the distal tubule and collecting duct. This reduces transepithelial voltage and impairs sodium-potassium exchange, leading to reduced potassium excretion and hyperkalemia.
Type IV renal tubular acidosis
Increased intake
High potassium diet, e.g., fresh fruits, dried fruits and legumes, vegetables, nuts, seeds, bran products, milk, and dairy products
K+ containing IV fluids
Extracellular shift
Extracellular release
Pathophysiology
Clinical features
Diagnostics
Initial : Serum potassium concentration > 5.0 mEq/L.
Must exclude pseudohyperkalemia (hemolysis during venipuncture, thrombocytosis, leukocytosis) via repeat non-traumatic blood draw.
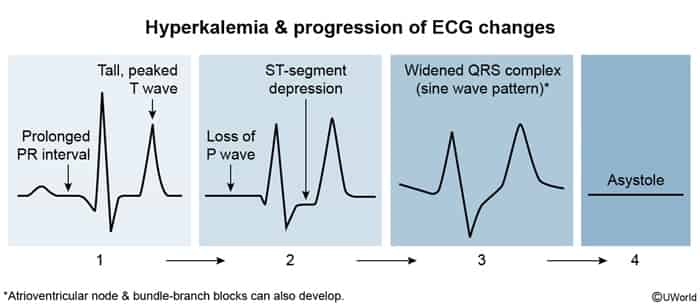
Crucial next step : 12-lead ECG to evaluate for cardiac toxicity.
Peaked T waves (earliest sign, narrow-based, symmetric).PR interval prolongation and flat/absent P waves.
QRS prolongation (widening).
Sine wave pattern (pre-arrest).
Key Labs:
BMP (evaluates BUN, Cr, HCO3-).
Digoxin level (if taking digoxin).
Creatine kinase (CK), urine myoglobin if rhabdomyolysis suspected.
Treatment
Scenario A: “Unstable” (ECG changes, palpitations, or severe K+ > 6.5-7.0)
Membrane Stabilization : IV Calcium Gluconate (or Calcium Chloride). c
Logic : Protects the heart from arrhythmia. Does NOT lower K+. Immediate onset.
Intracellular Shift (Temporizing) :
Insulin (Regular) + Dextrose (D50) : Most reliable shifter. Inhaled Beta-agonists (Albuterol) : High dose required.Sodium Bicarbonate: Only if acidosis is present.
Scenario B: “Stable” (No ECG changes, moderate elevation)
Eliminate K+ from the body (Definitive Management ).
Loop Diuretics (Furosemide) : If kidneys make urine.K+ Binders (Patiromer , Zirconium Cyclosilicate, Sodium Polystyrene Sulfonate): Slow onset (hours/days). c
Scenario C: Renal Failure/ESRD :
Hemodialysis : The definitive treatment for symptomatic hyperkalemia in dialysis patients.