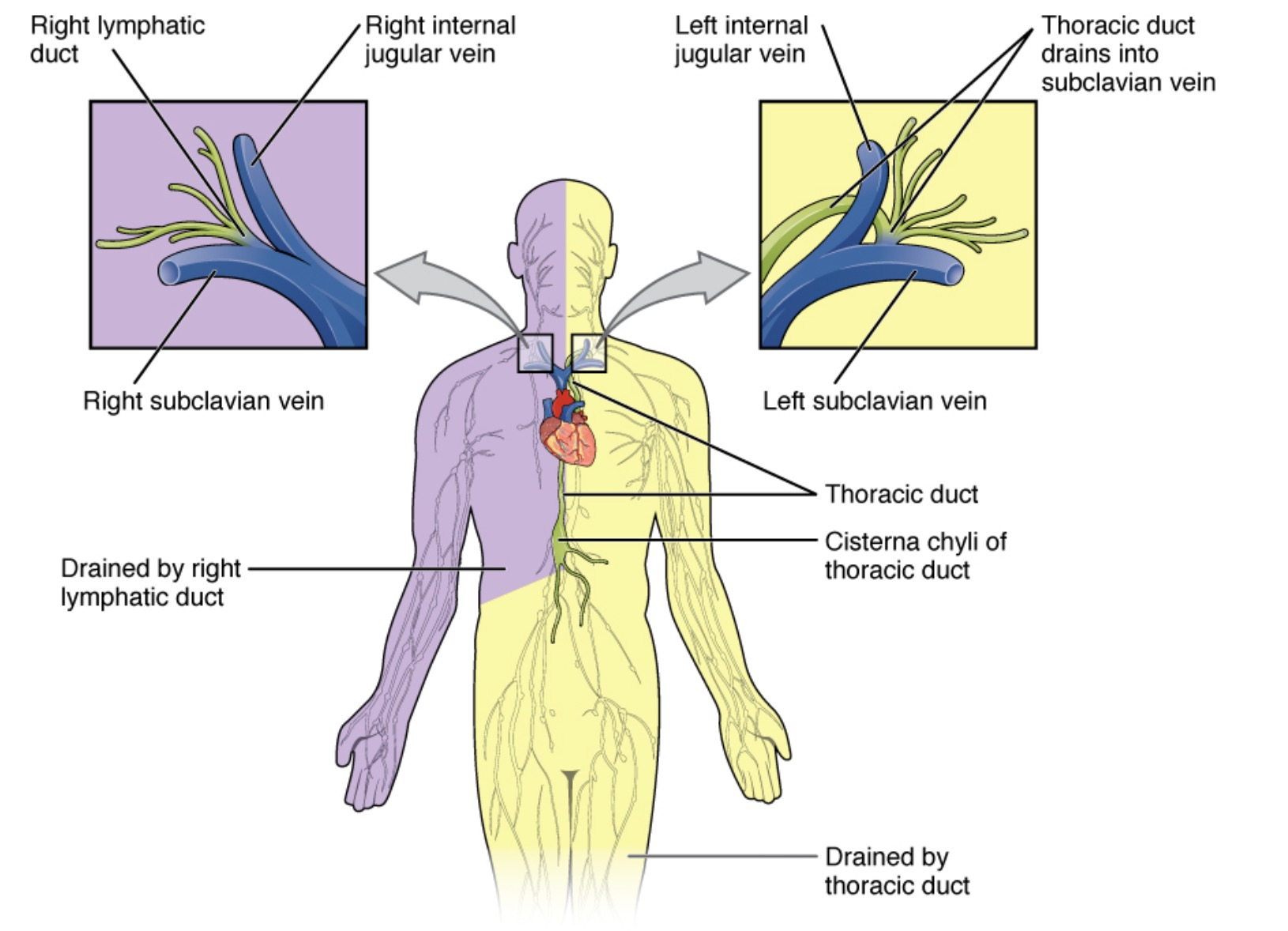
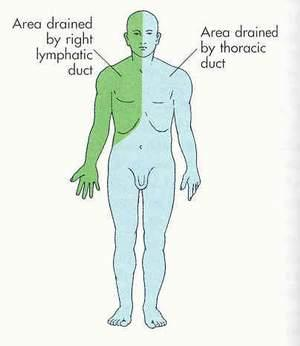
Right vs. Left Drainage: The right lymphatic duct drains the right side of the head, neck, right arm, and right thorax. The thoracic duct drains everything else (~75% of the body) and empties into the junction of the left subclavian and left internal jugular veins.
Anatomical Rule: In general, lymph drainage follows venous and arterial supply, especially in the GI tract.
Superficial vs. Deep: Lymphatics above the umbilicus generally drain to the axillary nodes, while those below the umbilicus drain to the superficial inguinal nodes.
Clinically Significant Nodes & Drainage Areas
Head and Neck
Cervical Nodes (Superficial/Deep): Drain the head and neck.
Clinical Correlate: Often enlarged in pharyngitis (e.g., strep throat, infectious mononucleosis), upper respiratory infections, and head/neck squamous cell carcinoma. t
Supraclavicular Nodes: Drain the thorax and abdomen.
Left Supraclavicular Node (Virchow’s Node): Receives drainage from the thoracic duct, which carries lymph from the abdominal cavity.
Buzzword:Troisier’s sign refers to a hardened, enlarged Virchow’s node.
Clinical Correlate: A classic sign of metastatic gastric cancer. It can also indicate other intra-abdominal malignancies like ovarian, testicular, or kidney cancer, as well as lymphoma.
Right Supraclavicular Node: Drains the mediastinum, lungs, and esophagus.
Clinical Correlate: Associated with thoracic malignancies such as lung and esophageal cancer, and Hodgkin’s lymphoma.
DDx for Supraclavicular Adenopathy: High suspicion for malignancy. Other causes include lymphoma, infections (especially TB, fungal), and sarcoidosis.
Thorax & Upper Limb
Axillary Nodes: Drain the upper limb, breast, and skin of the back/chest above the umbilicus.
Clinical Correlate: Crucial for staging breast cancer. Lymphatic drainage from the breast is primarily to the axillary nodes (~75%).
Surgical Levels (relative to pectoralis minor):
Level I: Lateral to the muscle.
Level II: Posterior to the muscle.
Level III: Medial to the muscle.
Sentinel Node Biopsy (SNB): A procedure to identify and remove the first lymph node(s) a tumor drains to, minimizing morbidity compared to full axillary dissection.
Internal Mammary Nodes: Drain the medial portion of the breast.
Abdomen & Pelvis
Celiac, Superior & Inferior Mesenteric Nodes: Drain their corresponding GI structures (stomach, small intestine, colon).
Para-aortic (Lumbar) Nodes: Drain the testes, ovaries, kidneys, and uterus.
Clinical Correlate: Primary site of metastasis for testicular cancer.
Lower Limb & Perineum
Superficial Inguinal Nodes: Drain most of the skin below the umbilicus, including the scrotum, vulva, and anal canal (below the pectinate line).
Exceptions: Does not drain the gonads (testes/ovaries) or the glans penis/clitoris.
Clinical Correlate: Enlarged in STIs (e.g., syphilis, chancroid, herpes), and lower extremity cellulitis.
Deep Inguinal Nodes: Drain the glans penis and clitoris.
Popliteal Nodes: Drain the dorsolateral foot and posterior calf.