Epidemiology
Etiology
- Viral: Most common cause (~70-90%). Adenovirus, Rhinovirus, Coronavirus, EBV (Mononucleosis), CMV, HSV.
- Bacterial: Group A -hemolytic Streptococcus (GAS/S. pyogenes) is the most important bacterial cause (15-30% in children). t
- Other Bacterial: Fusobacterium necrophorum (Lemierre syndrome), N. gonorrhoeae, C. diphtheriae (rare/unvaccinated).
Pathophysiology
Clinical features
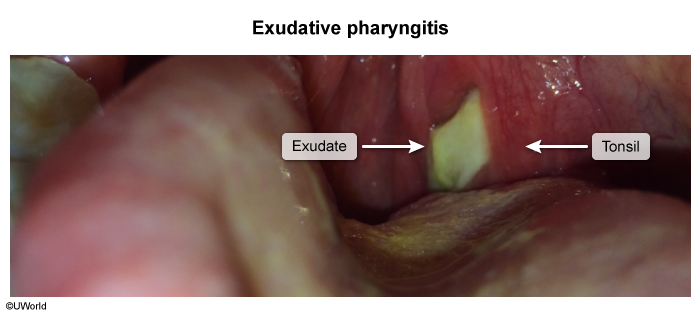
Acute bacterial tonsillopharyngitis
- Sudden onset of symptoms: fever, sore throat, dysphagia
- Significantly inflamed pharynx
- Pharyngeal and/or tonsillar erythema and edema
- Pharyngeal and/or tonsillar exudates (rare in children < 3 years of age)
- Fibrin deposits appear as white spots on the tonsils (杨梅舌). t
- See Gray-white exudates of throat
- Fibrin deposits appear as white spots on the tonsils (杨梅舌). t
- Palatal petechiae
- Cervical lymphadenitis
- Absence of cough
Acute viral tonsillopharyngitis
Accompanied by symptoms of a common cold (rhinitis and/or pharyngitis)
Diagnostics
Rapid strep test
- Modality: rapid antigen detection test (RADT) specific for GAS antigens.
- Indications: first-line test in suspected acute bacterial tonsillopharyngitis
- All symptomatic children ≥ 3 years of age and adults (unless symptoms are suggestive of acute viral tonsillopharyngitis)
- Procedure: Swab the patient’s tonsils and the back of the throat.
- Findings
- Identifies the presence of GAS (positive RADT).
- Time to result: 5–10 minutes
Additional laboratory tests
- Antistreptolysin O (ASO) titer
- Elevated levels suggest a previous GAS infection; not helpful to diagnose acute pharyngitis
- Indicated in the workup of nonsuppurative complications of GAS tonsillopharyngitis (e.g., acute rheumatic fever, PSGN).