Often asymptomatic or presents as a mononucleosis-like syndrome.
Symptoms include fever, malaise, myalgias, and atypical lymphocytosis.
A key distinguishing feature from EBV mononucleosis is the negative heterophile antibody (Monospot) test. Pharyngitis and significant lymphadenopathy are less common than in EBV.
At high risk for severe, end-organ disease, particularly when the CD4+ count is <50 cells/µL in AIDS patients.
Retinitis: The most common manifestation in advanced AIDS, presenting with hemorrhage and cotton-wool exudates on fundoscopy (“pizza pie” or “ketchup and mustard” appearance). Can lead to retinal detachment and blindness.
Colitis: Results in diarrhea, fever, and abdominal pain. Endoscopy often reveals ulcerations.
Esophagitis: Causes odynophagia (painful swallowing). Endoscopy typically shows large, linear ulcers in the distal esophagus.
Pneumonitis: A significant cause of morbidity and mortality in transplant recipients, especially after lung or hematopoietic stem cell transplants.
Encephalitis: Can occur in severely immunocompromised patients.
Congenital CMV
The most common congenital viral infection.
~90% of infected newborns are asymptomatic at birth.
Symptomatic newborns may present with hepatosplenomegaly, jaundice, thrombocytopenic purpura (“blueberry muffin” rash), microcephaly, and periventricular calcifications.
CMV is a leading cause of non-hereditary sensorineural hearing loss in children.
Diagnostics
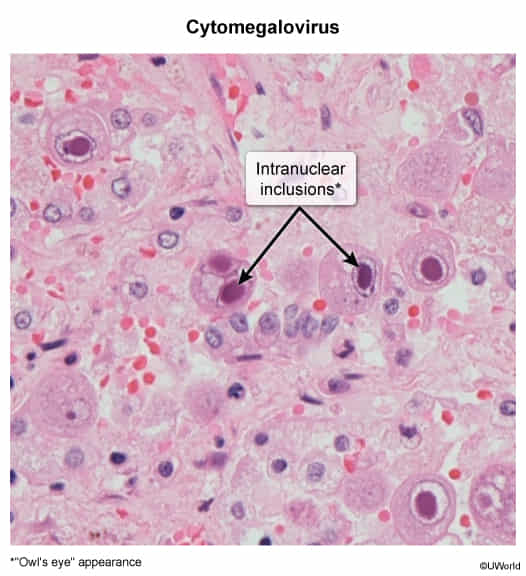
Histology: Enlarged cells with large, eosinophilic intranuclear inclusions surrounded by a clear halo (“owl’s eye” appearance).