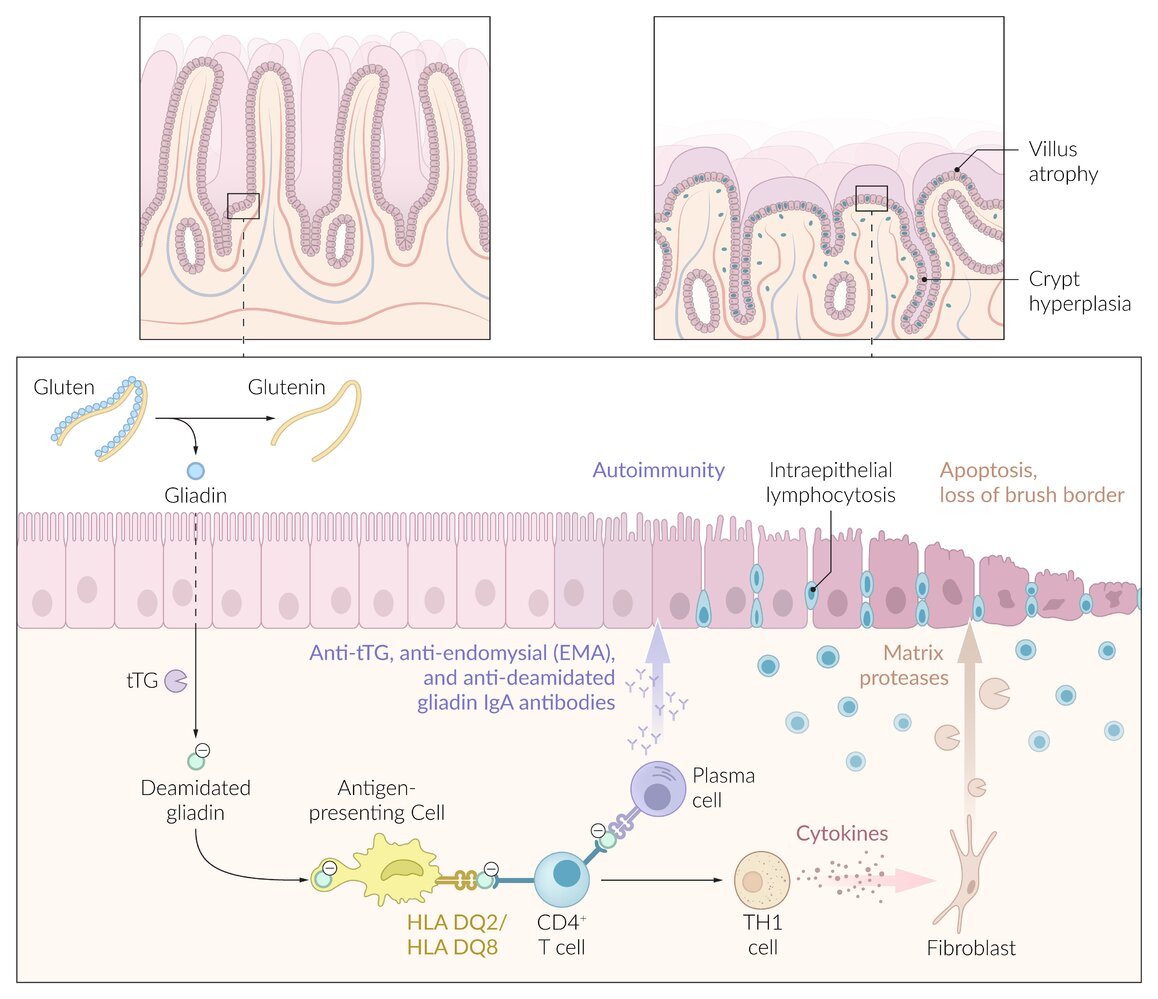
Gliadin reacts with transglutaminase (tTG) → deamidation of gliadin → presented by APCs via MHC Class II → Helper T-cell activation (Type IV Hypersensitivity).
Inflammation leads to mucosal damage primarily in the duodenum and proximal jejunum.t
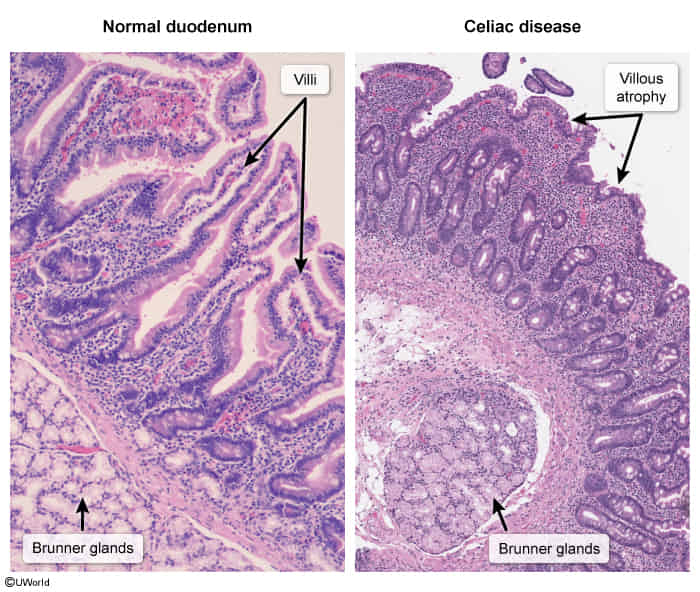
Histologic Damage: Chronic inflammation causes classic findings in the small bowel (duodenum/jejunum).
Villous atrophy: Blunting of villi leads to malabsorption.
Crypt hyperplasia: Compensatory lengthening of crypts. t
Intraepithelial lymphocytosis: Increased lymphocytes in the epithelial layer.
IgA tissue transglutaminase antibody (tTG IgA): initial testt
Total IgA
Indicated for all patients because of the high prevalence of IgA deficiency in patients with celiac disease (approx. 2–3%)
Both celiac disease and selective IgA deficiency have strong associations with specific HLA genes, particularly HLA-DQ2 and HLA-DQ8.
If patients have low IgA, perform further IgG-based testing.
Deamidated gliadin peptide
IgG-based testing: indicated in IgA deficiency or discordant biopsy and serology
IgG-tissue transglutaminase (tTG IgG)
IgG deamidated gliadin peptide (DGP IgG)
IgA-based testing: IgA deamidated gliadin peptide (DGP IgA)
Anti-endomysial antibody (EMA): Potential second-line confirmatory test (high-specificity)t
Celiac disease is not associated with elevated systemic inflammatory markers (eg, C-reactive protein, erythrocyte sedimentation rate), since it’s limited.t
Endoscopy
EGD with small intestine biopsy (confirmatory test)