Epidemiology & Risk Factors
Small Bowel Obstruction (SBO) :
Adhesions (prior surgery): #1 cause overall (60-70%). c Hernias: #2 cause overall; #1 cause in pts w/o surgical Hx.
Crohn disease c Malignancy: Primary or metastatic disease.
Intussusception : Common in pediatric pts.
Large Bowel Obstruction (LBO) :
Colorectal cancer : #1 cause overall.Volvulus: Sigmoid (elderly/institutionalized) or cecal (younger pts).
Diverticulitis: Chronic strictures.
Clinical Features
SBO :
Crampy, paroxysmal abdominal pain.
Early bilious vomiting (more prominent in proximal SBO).Abdominal distension (more prominent in distal SBO).
Obstipation (lack of flatus/stool; late finding).PE: High-pitched “tinkling” bowel sounds (early) or silent abdomen (late). Tympanitic abdomen. c
LBO :
Gradual onset of infraumbilical cramping pain.
Markedly distended abdomen.
Late/feculent vomiting (only if ileocecal valve is incompetent).
Early obstipation .
Diagnosis
Initial Test : Abdominal X-ray (AXR) (supine/upright).
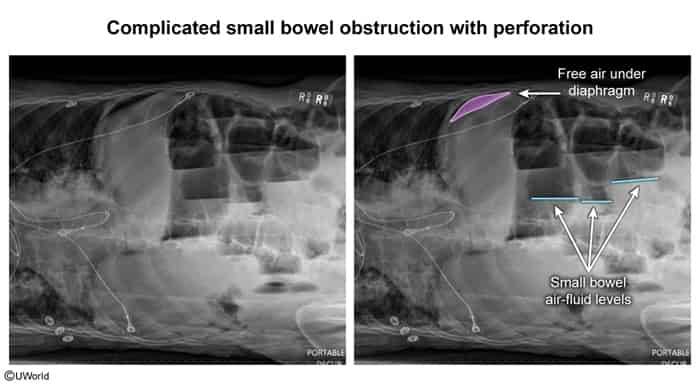
SBO findings: Dilated loops of small bowel (>3 cm), multiple air-fluid levels on upright view, absence of distal colonic gas.
LBO findings: Colonic dilation (>6 cm; cecum >9 cm).
Sigmoid Volvulus : “Coffee bean” sign arising from pelvis/LUQ.Cecal volvulus: Embryo/comma sign pointing to RUQ.
Best/Confirmatory Test : CT abdomen & pelvis w/ IV contrast .
Identifies transition point , etiology (e.g., mass, hernia), and complications.
Differentiates partial vs. complete obstruction.
Key Labs :
CBC: Leukocytosis (suggests ischemia, necrosis, or perforation).
BMP: Dehydration/electrolyte abnormalities (hypokalemic, hypochloremic metabolic alkalosis from vomiting; prerenal AKI ).
Serum lactate: Elevated levels suggest bowel ischemia.
Differential Diagnostics
Paralytic Ileus
Differentiating features: Uniformly dilated loops of both small & large bowel on AXR; absent bowel sounds; typically post-op or associated w/ hypokalemia or opioids .
Ogilvie Syndrome (Acute Colonic Pseudo-obstruction) :
Differentiating features: Massive colonic dilation without mechanical obstruction; occurs in critically ill/elderly pts; Rx with Neostigmine if refractory.
Mesenteric Ischemia
Differentiating features: Pain out of proportion to exam; typically presents w/ hematochezia, CV risk factors (AFib ), and lack of mechanical obstruction signs on CT.
Management
Initial Stabilization :
Make pt NPO (nil per os) immediately.
NGT decompression to suction.Aggressive IVF resuscitation (Normal Saline or Lactated Ringer’s) + electrolyte replacement.
Monitor urine output (Foley catheter).
Conservative/Non-operative Management :
Indicated for: Partial SBO , early post-op SBO, or uncomplicated Crohn-related SBO.
Regimen: Serial abdominal exams and imaging (AXR) every 12-24 hours.
Surgical Intervention :
Emergent Exploratory Laparotomy/Laparoscopy :
Indicated immediately for signs of complicated obstruction (strangulation, ischemia, necrosis, perforation):
Peritoneal signs (rebound tenderness, guarding, rigidity ).
Hemodynamic instability/shock .
Fever, persistent tachycardia, leukocytosis.
Pneumoperitoneum (free air under diaphragm ) on AXR/CT.
Urgent/Scheduled Surgery :
Indicated for complete mechanical obstruction that fails to resolve w/ conservative management after 24-48 hours.
Complications
Bowel ischemia/infarction.
Bowel perforation & peritonitis.
Intra-abdominal abscess.
Sepsis/septic shock & MODS.
Aspiration pneumonia.∂