Pathophysiology
Colorectal carcinogenesis pathways (molecular pathology)
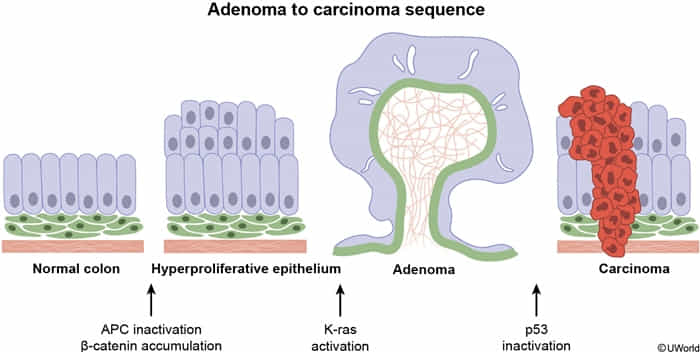
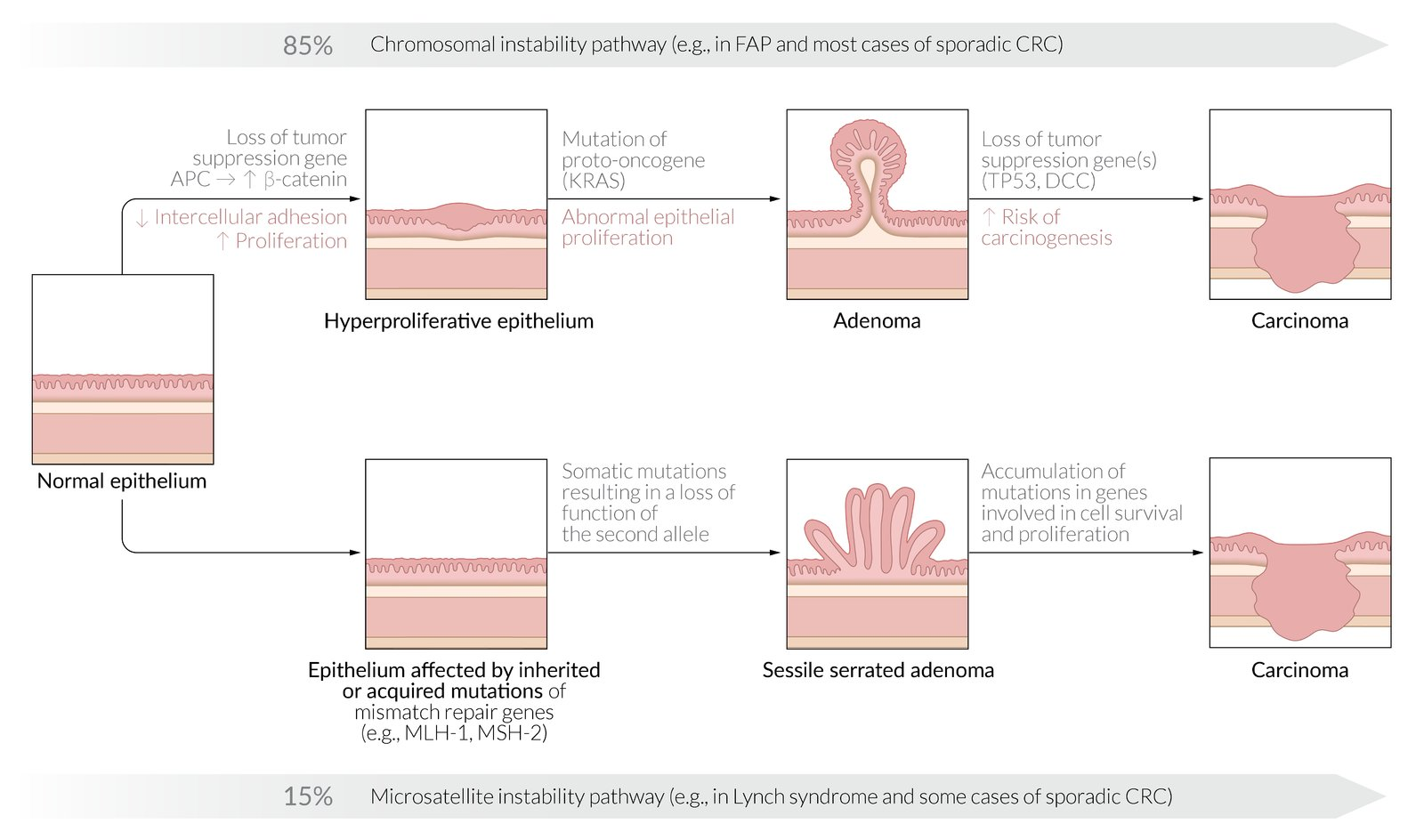
- 1. Chromosomal Instability (CIN) Pathway (~80%)
- The classic Adenoma-to-Carcinoma Sequence.
- Stepwise accumulation of key mutations:
- APC loss (initiation, ↑β-catenin)
- KRAS mutation (unregulated growth)
- p53 loss (malignancy)
- Clinical Association:
- Sporadic CRC (most common).
- Familial Adenomatous Polyposis (FAP): Germline mutation in APC.
Mnemonic
This follows the alphabet: APC -> KRAS -> P53
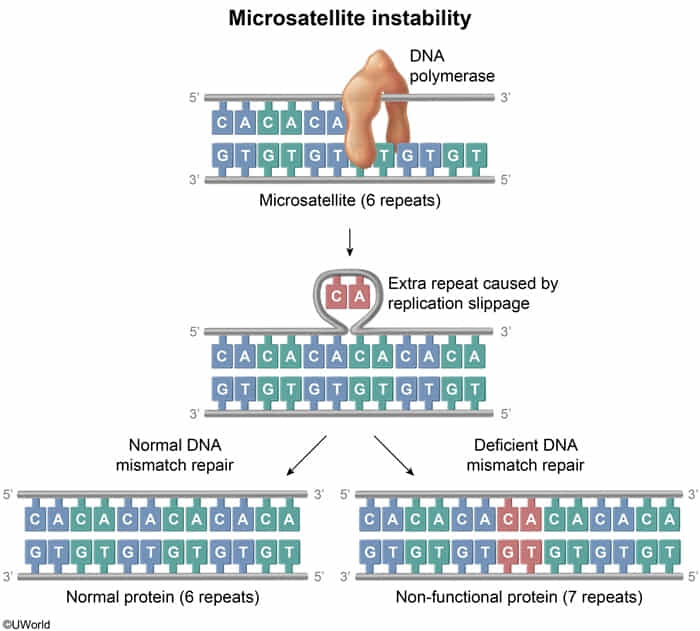
- 2. Microsatellite Instability (MSI) Pathway (~15%)
- Caused by defective DNA Mismatch Repair (MMR).
- Microsatellites are short, repetitive DNA sequences (e.g., CACACA…). During DNA replication, these regions are prone to errors (insertions/deletions).
- Due to mutations in MLH1, MSH2, MSH6, PMS2.
- Leads to errors in repetitive DNA sequences (microsatellites).
- Associated with Lynch Syndrome (HNPCC) and right-sided tumors.
- 3. Serrated Pathway (~5%)
- Arises from serrated polyps.
- Driven by BRAF mutation followed by CIMP (CpG Island Methylator Phenotype).
- CIMP hypermethylates and silences genes, often including the MLH1 mismatch repair gene, which can lead to MSI.
- COX-2 overexpression
Epidemiology & Risk Factors
- Age ≥ 45 (standard screening starts at 45 for average risk).
- Inherited syndromes: FAP (APC mutation, 100% progress to CRC), Lynch syndrome (MMR gene mutation, MSI).
- Personal/family history of CRC or adenomatous polyps.
- IBD (UC carries higher risk than Crohn’s disease; risk increases with duration and extent of disease).
- Pathogens: Streptococcus bovis, Clostridium septicum c
- Modifiable: High red/processed meat diet, low fiber, obesity, smoking, alcohol. c
- Heme iron (abundant in red meat) catalyzes the Fenton reaction, generating reactive oxygen species (ROS).
| Syndrome | Gene Mutation | Colon Cancer Risk | Other Associated Neoplasms |
|---|---|---|---|
| Familial adenomatous polyposis | APC | 100% | Upper gastrointestinal, Thyroid, Desmoids/osteomas |
| Lynch syndrome | MSH2/6, MLH1 | 50%-80% | Endometrial, Ovarian |
| Peutz-Jeghers syndrome | STK11 | 39% | Upper gastrointestinal, Pancreatic, Breast |
| Characteristics | Colitis-associated | Sporadic |
|---|---|---|
| Age | Younger (age 40-55) | Older (age >60) |
| Origin of dysplasia | Flat (nonpolypoid) lesions | Polypoid lesions |
| Location | Proximal > distal (particularly with CD) | Distal > proximal |
| Tumors | Multifocal | Singular |
| Histology | Mucinous and/or signet ring cells, Poorly differentiated | Rarely mucinous, Well differentiated |
| Mutations | Early p53 mutation, Late APC gene mutation | Early APC gene mutation, Late p53 mutation |
Pathophysiology
Clinical features
Right-sided colon carcinomas
- Large, bulky masses that protrude into the colonic lumen due to the relatively large caliber of the ascending colon
- Occult bleeding or melena
- Manifestations of iron deficiency anemia (due to chronic bleeding)
Left-sided colon carcinomas
- Often infiltrate the wall of the colon, encircling it and narrowing the lumen
- More likely to cause obstruction
- Changes in bowel habits (size, consistency, frequency)
- Blood-streaked stools
- Colicky abdominal pain (due to obstruction) c
- Bowel obstruction occurs earlier in left-sided colon carcinomas because the distal colon has a smaller lumen than the proximal colon and contains solid fecal matter.
Diagnostics
- Initial/Screening Options:
- Colonoscopy every 10 years (preferred, diagnostic & therapeutic).
- Fecal Immunochemical Test (FIT) or Fecal Occult Blood Test (FOBT) annually.
- A negative fecal occult blood test (guaiac-negative stool) does not rule out GI malignancy, as tumor bleeding is often intermittent. Scopes must still be performed.
- Multi-target stool DNA (Cologuard) every 3 years.
- Confirmatory/Gold Standard: Colonoscopy with biopsy showing adenocarcinoma.
- Staging & Workup:
- CT Chest/Abdomen/Pelvis to evaluate for metastatic disease.
- Pelvic MRI or Endorectal Ultrasound (EUS) specifically for rectal cancer (assesses depth of invasion & nodal status).
- Key Labs: Microcytic anemia (↓ Hb, ↓ MCV, ↓ ferritin).
- Tumor Marker: CEA (Carcinoembryonic Antigen). Crucial Note: Not used for screening or diagnosis; used solely for monitoring disease recurrence and response to treatment.
Treatment
- Colon Cancer (Stage I-III):
- Surgical Resection: Upfront partial colectomy (hemicolectomy) with wide margins and regional lymphadenectomy (min 12 LNs required for staging).
- Adjuvant Chemotherapy: Indicated for Stage III (node-positive) and high-risk Stage II. Regimen: FOLFOX (5-FU, Leucovorin, Oxaliplatin) or CAPOX.
- Rectal Cancer (Stage II-III):
- Neoadjuvant Therapy: Chemoradiotherapy (5-FU + radiation) to downstage tumor before surgery.
- Surgical Resection: Total mesorectal excision (TME).
- Low Anterior Resection (LAR): For upper/middle rectal tumors; allows sphincter preservation.
- Abdominoperineal Resection (APR): For lower rectal tumors invading sphincter; requires permanent colostomy.
- Adjuvant Chemotherapy: Completed post-operatively.
- Metastatic Disease (Stage IV):
- If isolated resectable mets, esp liver/lung:
- Resection or ablation + systemic chemo can be curative-intent. c
- Unresectable/metastatic:
- Systemic chemo: FOLFOX, FOLFIRI, or CAPOX
- Add biologic depending on markers:
- Bevacizumab: anti-VEGF
- Cetuximab/panitumumab: only RAS wild-type, usually left-sided tumors
- Pembrolizumab/nivolumab: MSI-H/dMMR metastatic CRC
- If isolated resectable mets, esp liver/lung:
Follow-up
- Patient history, physical examination, CEA level
- Every 3–6 months for 2 years
- Every 6 months for an additional 3 years
- CT chest/abdomen/pelvis: annually for 5 years
- Colonoscopy
- 1 year after preoperative colonoscopy c
- Every 3–5 years in the further follow-up, depending on findings
- Proctoscopy/sigmoidoscopy
- Recommended additional follow-up modality after the treatment of rectal cancer
- Every 6–12 months for 3–5 years
- May be supplemented with endorectal ultrasound
- Recommended duration of close follow-up: 5 years following the completion of curative treatment
Screening
Average-Risk CRC Screening Guidelines
- Screening Initiation: Begin routine screening at age 45 years (recently lowered from 50).
- Screening Termination:
- Ages 45–75 years: Strong recommendation for routine screening.
- Ages 76–85 years: Individualize based on comorbidities, life expectancy (>10 years), and prior screening history.
- Ages >85 years: Discontinue screening.
- Screening Modalities & Standard Intervals:
- Colonoscopy: Every 10 years (Gold standard / Tier 1 option; both diagnostic and therapeutic). c
- Fecal Immunochemical Test (FIT): Annually (Tier 1 option).
- High-sensitivity Guaiac FOBT (gFOBT): Annually.
- Multi-target stool DNA (mt-sDNA / Cologuard): Every 3 years.
- CT Colonography or Flexible Sigmoidoscopy: Every 5 years.
- Key Step 2 CK Rule: Any positive result on a non-colonoscopy screening test (FIT, gFOBT, mt-sDNA, CT colonography) must be followed by a diagnostic colonoscopy within 6 months. c
High-Risk CRC Screening Protocols
- Family History of CRC or Advanced Adenoma:
- ≥1 First-Degree Relative (FDR) diagnosed at <60 years (or ≥2 FDRs at any age): Begin screening at age 40 or 10 years before the youngest relative’s diagnosis (whichever is earlier). Perform screening with colonoscopy only and repeat every 5 years. c
- 1 FDR diagnosed at age ≥60 years: Begin screening at age 40. Screening intervals and modalities are the same as average-risk populations (e.g., colonoscopy every 10 years or annual FIT).
- Inflammatory Bowel Disease (IBD - UC or Crohn’s with colitis):
- Begin surveillance colonoscopy 8 years after symptom onset.
- Repeat colonoscopy every 1–3 years with random/targeted biopsies. c
- Lynch Syndrome (HNPCC):
- Autosomal dominant mismatch repair (MMR) gene mutation.
- Begin screening colonoscopy at age 20–25 years (or 2–5 years before the youngest family diagnosis).
- Repeat colonoscopy every 1–2 years.
- Familial Adenomatous Polyposis (FAP):
- Autosomal dominant APC gene mutation.
- Begin screening with annual sigmoidoscopy/colonoscopy at age 10–12 years.
- Management: Prophylactic colectomy once carpeted polyposis is identified.
- Prior Childhood Cancer (Radiation Therapy):
- History of abdominopelvic or total body irradiation.
- Begin colonoscopy starting at age 30 or 5 years after radiation (whichever is last). Repeat every 5 years.
Post-Polypectomy Surveillance Intervals
All surveillance intervals assume a complete exam, adequate bowel preparation, and complete resection of all identified polyps.
Low-Risk Polyp Findings
- Distal hyperplastic polyps <10 mm: Regarded as normal. Repeat screening in 10 years.
- 1–2 small (<10 mm) tubular adenomas: Repeat colonoscopy in 7–10 years (under updated guidelines).
- 1–2 small (<10 mm) sessile serrated polyps (SSPs): Repeat colonoscopy in 5–10 years.
Intermediate/High-Risk Polyp Findings
- 3–4 small (<10 mm) tubular adenomas or SSPs: Repeat colonoscopy in 3–5 years.
- 5–10 tubular adenomas or SSPs: Repeat colonoscopy in 3 years.
- Advanced Adenomas (defined as ≥10 mm, villous/tubulovillous histology, or high-grade dysplasia [HGD]): Repeat colonoscopy in 3 years.
- High-Risk SSPs (defined as ≥10 mm or SSP with dysplasia): Repeat colonoscopy in 3 years.
- >10 adenomatous polyps (or SSPs) in a single session: Repeat colonoscopy in 1 year (work up for underlying polyposis syndromes).
Large Polyps & Piecemeal Resection
- Large polyps (≥2 cm) removed via piecemeal resection: High risk of local recurrence. Repeat colonoscopy in 6–12 months. If no recurrence, repeat in 1 year, then in 3 years.
Surveillance after Negative Follow-up
- If surveillance colonoscopy is negative following prior low-risk findings: Repeat colonoscopy in 10 years.
- If surveillance colonoscopy is negative following prior high-risk findings: Repeat colonoscopy in 5 years.