Hepatitis C is most associated with hepatocellular carcinoma in the United States t
Needle sharing…?
Pathophysiology
Clinical features
Diagnostics
Screening: RUQ US + AFP every 6 months for high-risk patients (cirrhotics, select HBV carriers).
Initial/Best Imaging: Triple-phase contrast CT or MRI of the abdomen.
Diagnostic findings: Arterial phase enhancement (hypervascularity) followed by rapid venous washout (delayed portal venous phase).
Key Labs: Elevated AFP (typically > 20 ng/mL; values > 400 ng/mL in a cirrhotic patient are highly specific).
At the commonly used 20 ng/mL threshold, AFP demonstrates a sensitivity of approximately 60% and specificity of approximately 84-90%c
Biopsy: Generally avoided in cirrhotic patients with classic imaging findings (arterial enhancement + washout) due to the risk of tumor seeding along the needle tract. Only indicated if imaging is atypical or the liver is non-cirrhotic.
Differential diagnostics
Metastatic liver disease
Most common malignant liver lesion
Typical primary tumor sites: gastrointestinal tract (colon, stomach, pancreas), lung, and breast
The most common cause of liver metastases is colorectal cancer, which spreads directly from the colon or superior rectum through the portal venous system to the liver.
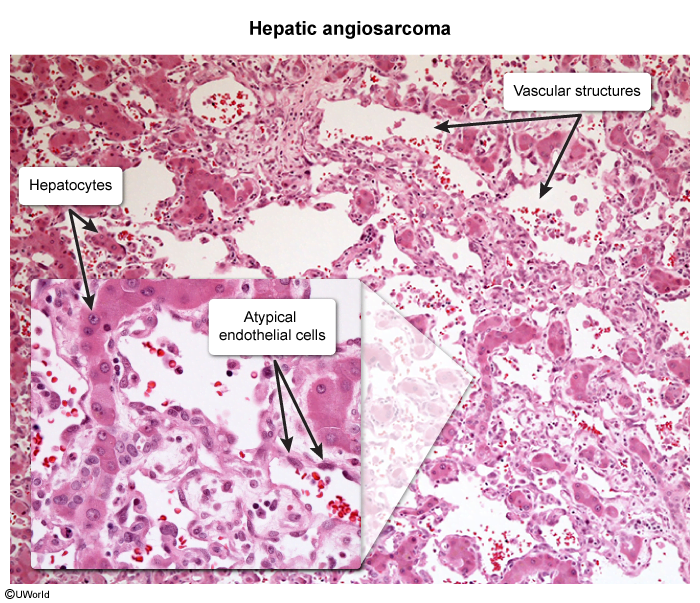
Hepatic angiosarcoma
Etiology: associated with exposure to vinyl chloride, arsenic, or thorium dioxide