Postoperative state: Most common cause of postoperative ileus (POI); transient impairment of bowel motility is expected after abdominal surgery (typically resolves in 3-5 days).
Electrolyte abnormalities: Severe hypokalemia, hypomagnesemia, hypercalcemia.
Diffuse, dull, constant abdominal discomfort (typically painless compared to the colicky pain of mechanical obstruction). c
Nausea, obstipation, inability to tolerate oral intake, and bilious vomiting.
Inability to pass flatus or stool.
Physical Exam:
Distended, tympanitic abdomen.
Absent or hypoactive bowel sounds (differs from early mechanical obstruction which has hyperactive/tinkling sounds).
No localized peritoneal signs unless complicated by ischemia or perforation.
Diagnosis
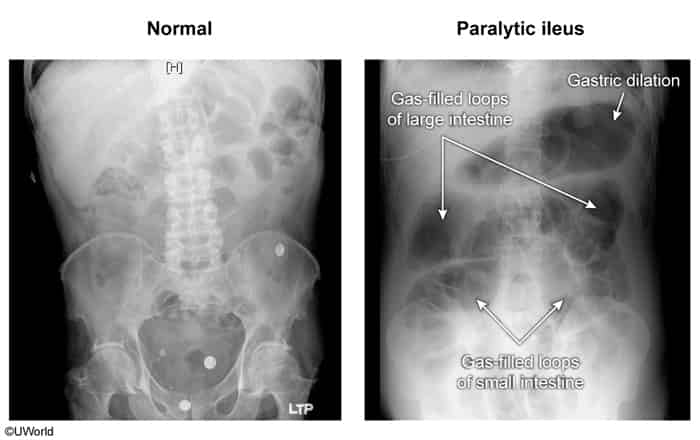
Initial: Abdominal X-ray (XR).
Shows uniformly dilated loops of both small and large bowel with gas present in the rectum.
Small bowel obstruction would demonstrate only dilated loops of small bowel (without dilated loops of large bowel) on x-ray
Absence of a transition point.
Key Labs:
BMP (assess for hypokalemia, hypomagnesemia, and AKI/dehydration).
CBC (evaluate for leukocytosis indicating underlying infection or ischemia).
Confirmatory/Gold Standard: Abdominal CT with oral and IV contrast.
Differentiates ileus from mechanical obstruction.
Shows diffuse bowel dilation without a mechanical transition point.
Differential Diagnostics
Small Bowel Obstruction (SBO): Differs by presenting with severe, colicky abdominal pain, hyperactive or high-pitched “tinkling” bowel sounds early, XR showing air-fluid levels with minimal/no distal rectal gas, and CT showing a clear transition point.
Ogilvie Syndrome (Acute Colonic Pseudo-obstruction): Differs by dilation limited primarily to the colon (cecum and ascending colon), often associated with normal or hyperactive bowel sounds; cecal diameter > 9-12 cm carries high risk of perforation.
Large Bowel Obstruction (LBO): Differs by mechanical blockage (e.g., neoplasm, volvulus), CT shows transition point and massive proximal colonic dilation with decompression distally.
Bowel rest (NPO) and maintenance/resuscitative IVF.
Aggressive correction of electrolytes (especially target K+ > 4.0 mEq/L and Mg2+ > 2.0 mg/dL).
Discontinue/minimize offending medications (e.g., transition from opioids to NSAIDs/acetaminophen).
Early mobilization to stimulate GI motility.
Decompression:
Nasogastric (NG) tube placement for patients with intractable vomiting or severe abdominal distension to prevent aspiration.
Pharmacotherapy (Refractory POI):
Alvimopan (peripherally acting mu-opioid receptor antagonist) for POI prevention in patients undergoing bowel resection.
Metoclopramide or erythromycin (prokinetics) have limited efficacy but may be trial-tested in refractory cases without mechanical obstruction.
Complications
Aspiration pneumonia secondary to severe vomiting and gastric distension.
Dehydration and AKI from third-spacing of fluids into the bowel lumen.
Bowel ischemia/perforation (rare, but possible if massive distension persists untreated).
Malnutrition if ileus is prolonged (> 7 days).
Postoperative Ileus
Epidemiology & Risk Factors
Normal physiological response to abdominal surgery (typically resolves in 24–72 hours); becomes pathological (prolonged ileus) if it persists >3–5 days.
Risk Factors:
Abdominal or pelvic surgery (due to direct bowel manipulation).