Epidemiology
Etiology
- Inflammatory Bowel Disease (IBD): Most common cause; Ulcerative Colitis (UC) > Crohn’s Disease (CD).
- Infectious Colitis: Particularly Clostridioides difficile (pseudomembranous colitis), CMV (in HIV/immunosuppressed pts), Salmonella, Shigella, Campylobacter.
- Precipitating Factors: Use of antimotility agents (e.g., loperamide), anticholinergic/narcotic drugs, barium enema, or recent colonoscopy during an acute flare.
Pathophysiology
- Colonic accumulation of inflammatory mediators and bacteria → nitric oxide synthesis → colonic dilation
- Edema and inflammation of the colonic smooth muscle → colonic dysmotility → colonic dilation
Clinical features
- Toxic appearance: fever >38°C, tachycardia, hypotension.
- Abdominal distension + pain/tenderness.
- Bloody diarrhea (in IBD) or watery diarrhea (in C. diff); May paradoxically ↓ as colon dilates → ominous sign. c
- AMS, dehydration.
- Peritoneal signs → suggests perforation (surgical emergency).
Diagnostics
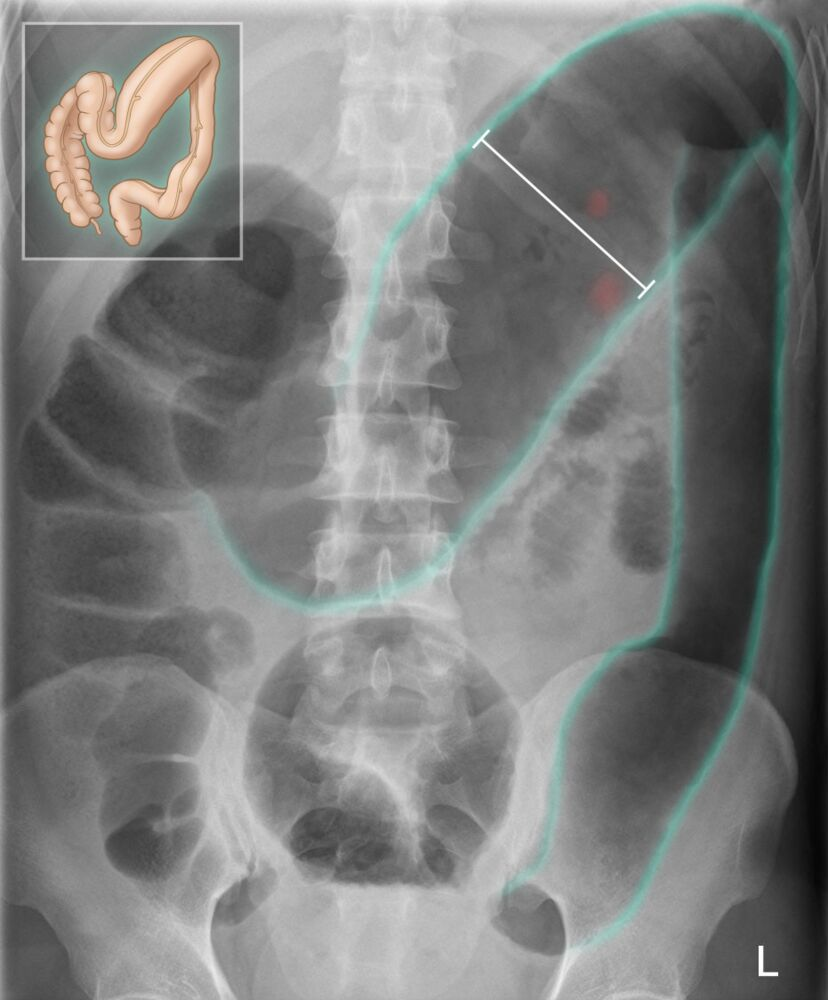
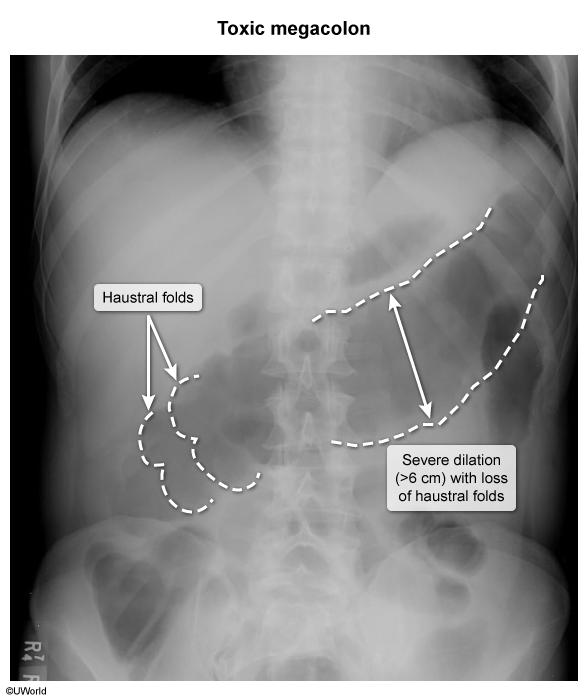
- Initial & Diagnostic Imaging: Plain abdominal radiograph (KUB) showing colonic dilation (typically transverse colon > 6 cm) w/ loss of haustral markings (“thumbprinting” due to mucosal edema).
Warning
Colonoscopy should be avoided in patients with suspected toxic megacolon since it increases the risk of colonic perforation.
Treatment
- First-line (Stabilization & Conservative):
- Make pt strictly NPO; insert nasogastric tube (NGT) for gastric decompression.
- Aggressive IVF resuscitation and correction of electrolyte abnormalities (especially hypokalemia to prevent worsening ileus).
- Discontinue all offending agents: Anticholinergics, antimotility drugs, and opiates.
- Medical Therapy (Etiology-specific):
- Broad-spectrum IV antibiotics (e.g., Ceftriaxone + Metronidazole, or Piperacillin-Tazobactam) to cover enteric pathogens and prevent translocation/sepsis.
- IBD-induced: IV corticosteroids (e.g., Methylprednisolone). c
- C. diff-induced: Oral Vancomycin (via NGT or retention enema if ileus present) + IV Metronidazole.
- Refractory/Surgical:
- Emergency subtotal colectomy with end ileostomy if no clinical improvement within 24–72 hours of medical therapy, or immediately if bowel perforation, peritonitis, or massive hemorrhage occurs. c