Decreased stool frequency or inability to pass flatus/stool.
Paradoxical diarrhea (liquid stool bypasses the obstructing fecal mass; often misdiagnosed as infectious diarrhea). c
Vague lower abdominal pain, distension, tenesmus, and anorexia.
Urinary retention or frequency (due to extrinsic compression on bladder/urethra).
Physical Exam:
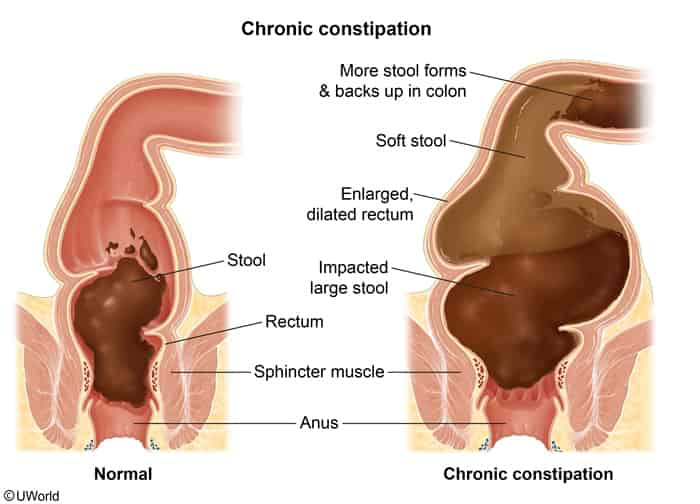
Digital Rectal Exam (DRE): Palpable hard, dry, impacted stool in the rectal vault.
Abdomen: Distended, tympanitic, sometimes a palpable firm left lower quadrant mass. Mild tenderness, but peritonitis is absent unless perforation has occurred.
Diagnosis
Initial: Digital Rectal Exam (DRE). Diagnostic for low/distal impaction.
Imaging:
Abdominal X-ray (XR): Indicated if DRE is negative but clinical suspicion remains high (evaluates for high/proximal impaction). Shows large amounts of stool in the colon, megacolon, or dilated bowel loops with air-fluid levels.
Abdominal CT: Reserved for cases with suspected complications (e.g., perforation, stercoral colitis) or to rule out a mechanical mass (e.g., colorectal cancer).
Key Labs: Generally normal. Check BMP if severe vomiting/dehydration (hypokalemia, acute kidney injury) or to rule out hypercalcemia/hypothyroidism as a cause of constipation.
Management
Manual Disimpaction:
First-line for distal/rectal impactions.
Perform gently using lubricated, gloved finger. May use topical lidocaine jelly to reduce discomfort.
Enemas & Suppositories:
Indicated after manual disimpaction or if stool is out of reach of manual extraction.
Use mineral oil enemas (to lubricate) or warm water/phosphate enemas (to stimulate motility).
Note: Avoid phosphate enemas in elderly or renal insufficiency due to risk of hyperphosphatemia.
Polyethylene glycol (PEG) is highly effective once the distal rectum is cleared.
Contraindication: Do NOT give oral laxatives (especially osmotic/stimulant) if complete distal obstruction is present, as it can cause severe abdominal cramping, vomiting, or perforation.
Prevention:
Increase dietary fiber, fluid intake, and physical activity.
Minimize constipating medications; use prophylactic bowel regimens if opioids are mandatory (e.g., senna + docusate, methylnaltrexone).