Etiology
- Genetic predisposition with association to HLA antigens
- Consuming gliadin from grains such as wheat, rye, and barley leads to an autoimmune reaction within the small intestinal wall.
- Associated conditions:
- Type 1 DM, autoimmune thyroiditis. c
- Down, Turner, and Williams syndromes.
- Selective IgA deficiency.
- First-degree relatives.
Pathophysiology
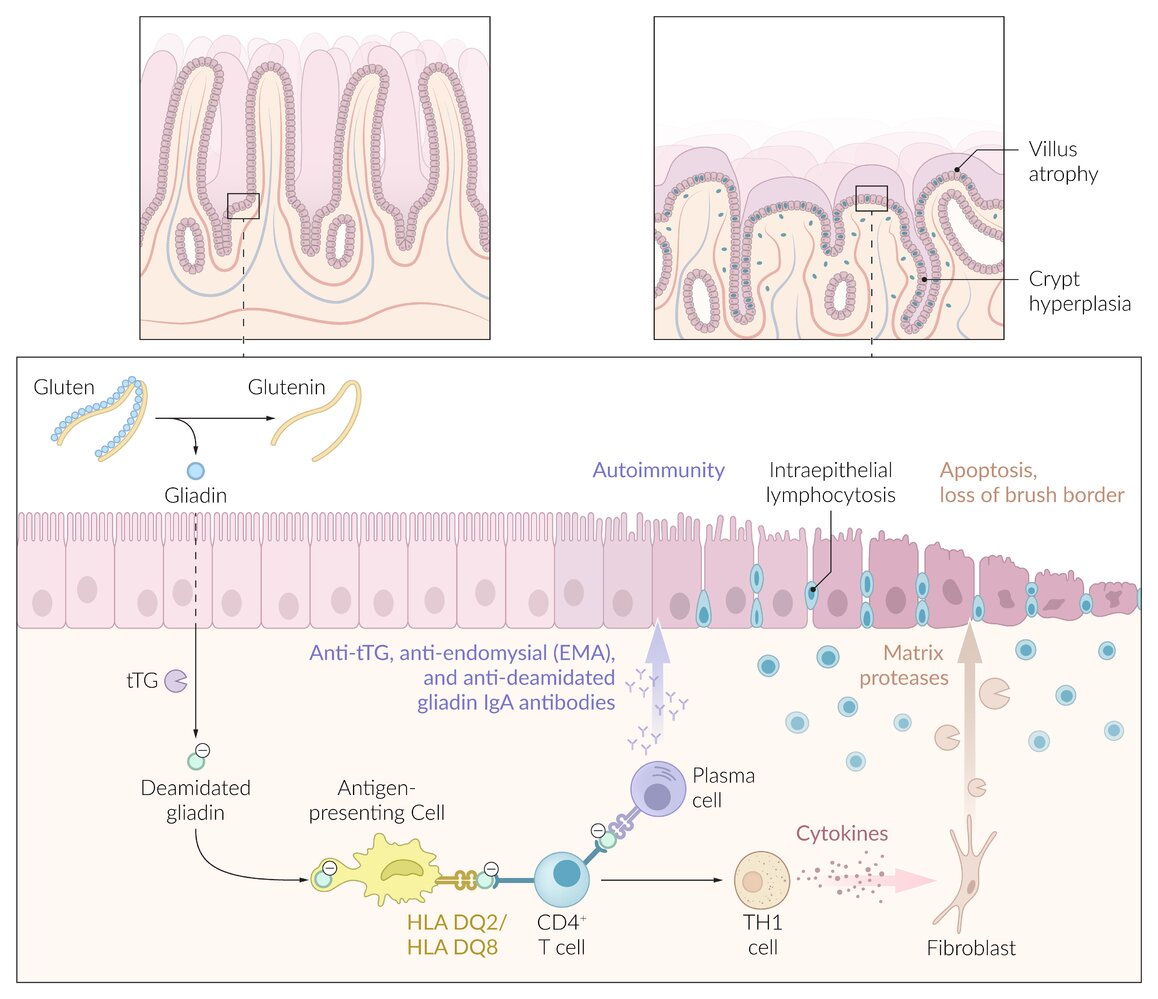
- Autoimmune-mediated intolerance of gliadin (gluten protein found in wheat, barley, rye).
- HLA-DQ2 (95%) and HLA-DQ8 associations.
- Gliadin reacts with transglutaminase (tTG) → deamidation of gliadin → presented by APCs via MHC Class II → Helper T-cell activation (Type IV Hypersensitivity).
- Inflammation leads to mucosal damage primarily in the duodenum and proximal jejunum. t
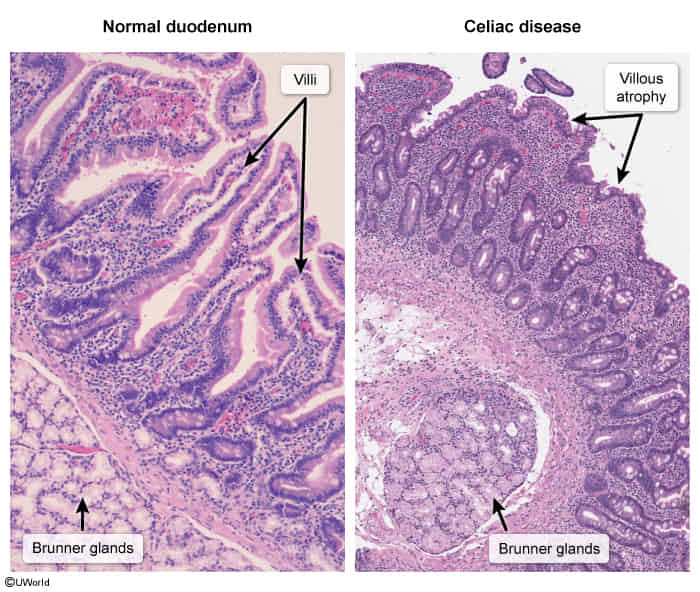
- Histologic Damage: Chronic inflammation causes classic findings in the small bowel (duodenum/jejunum).
- Villous atrophy: Blunting of villi leads to malabsorption.
- Crypt hyperplasia: Compensatory lengthening of crypts. t
- Intraepithelial lymphocytosis: Increased lymphocytes in the epithelial layer.
Clinical features
- GI Sx: Chronic diarrhea, steatorrhea (foul-smelling, floating stools), bloating, abdominal pain.
- Extraintestinal Sx:
- Dermatitis herpetiformis: Pruritic, papulovesicular rash on extensor surfaces (pathognomonic; due to IgA deposition at dermal papillae).
- Iron deficiency anemia (due to ↓ iron absorption in duodenum, not blood loss).
- Failure to thrive (peds), weight loss. c
- Osteopenia/Osteoporosis (↓ Vit D/Ca absorption).
- Neuro Sx (peripheral neuropathy). c
- Atrophic Glossitis: Malabsorption of key micronutrients (iron, folate, B-vitamins) leads to mucosal atrophy of the tongue. c
Tip
In both children and adults, mild or asymptomatic cases are more common than the classic presentation of the disease.
Diagnostics
Laboratory studies
- Anti-tissue transglutaminase (tTG) IgA AND total serum IgA (essential to r/o selective IgA deficiency; if IgA deficient, use IgG tTG or IgG deamidated gliadin peptide [DGP]). c
- There is a strong association between CD and selective IgA deficiency. In that case, IgA-based serologies will be falsely negative c
- Anti-endomysial IgA (high specificity, lower sensitivity than tTG IgA).
- Note: Diagnostic testing must be performed while the Pt is on a gluten-containing diet (false negatives on GFD).
- Celiac disease is not associated with elevated systemic inflammatory markers (eg, C-reactive protein, erythrocyte sedimentation rate), since it’s limited. t
- Key Labs: Fe-deficiency anemia, ↓ ferritin, ↓ Ca, ↓ Vit D, ↓ albumin, ↑ ALP, prolonged PT (Vit K malabs).
Endoscopy
- EGD with small intestine biopsy (confirmatory test)
- Intraepithelial lymphocytic infiltration
- Crypt hyperplasia
- Villous atrophy
Differential diagnostics
Comparison of Common GI Disorders
Link to original
Feature Celiac Disease Crohn Disease Tropical Sprue Lactose Intolerance Irritable Bowel Syndrome (IBS) Patho Autoimmune vs. Gliadin (HLA-DQ2/8) Transmural inflammation (Th1 mediated) Post-infectious; affects entire small bowel Lactase enzyme deficiency Gut-brain axis d/o; visceral hypersensitivity Location Proximal Small Bowel (Duodenum) Anywhere (“mouth to anus”); Terminal Ileum common Entire Small Bowel Small Intestine Brush Border Colon (Function, not structure) Biopsy Villous atrophy, crypt hyperplasia Non-caseating granulomas, transmural inflammation Villous atrophy (less severe) Normal Normal KeyDx ↑ Anti-tTG Ab; Dermatitis herpetiformis Skip lesions, “cobblestoning”, fistulas Hx of travel to tropics; Folate/B12 def. H2 breath test; symptoms with dairy Pain relieved by defecation; Dx of exclusion Tx Gluten-free diet Anti-TNF, Corticosteroids, 5-ASA Antibiotics, Folic Acid Avoid dairy; lactase pills Low FODMAP diet, fiber, symptom control
Tropical sprue
- Definition: A disease characterized by chronic diarrhea with subsequent malabsorption in association with a stay in the tropics or subtropics.
- Epidemiology: occurs in residents of the tropics and subtropics or in travelers returning from these areas (after trips lasting several weeks)
- Etiology: exact cause not known; most likely due to bacterial infection that leads to structural damage of the intestinal mucosa
- Clinical features: similar to Celiac disease
- Diagnostics
- Endoscopy of the small bowel and biopsy: villous atrophy, elongated crypts, presence of inflammatory cells (plasma cells, lymphocytes, eosinophils)
- Treatment: tetracycline in combination with folic acid for 3–6 months
Treatment
- Strict, lifelong gluten-free diet
- Abstain from products containing wheat, rye, barley, or spelt.
- Symptoms usually improve quickly