Definition
- Systemic vasculitis of medium-sized vessels and small muscular arteries, leading to tissue ischemia
- Most commonly involves the skin, peripheral nerves, muscles, joints, gastrointestinal tract, and kidneys
Epidemiology
- Peak incidence: 45–65 years of age
- Sex: ♂ > ♀
Etiology
- A third of patients have underlying viral hepatitis B or hepatitis C.
- In these individuals, PAN is likely triggered by the deposition of immune complexes (viral antigen bound by host antibody) in the arterial wall.
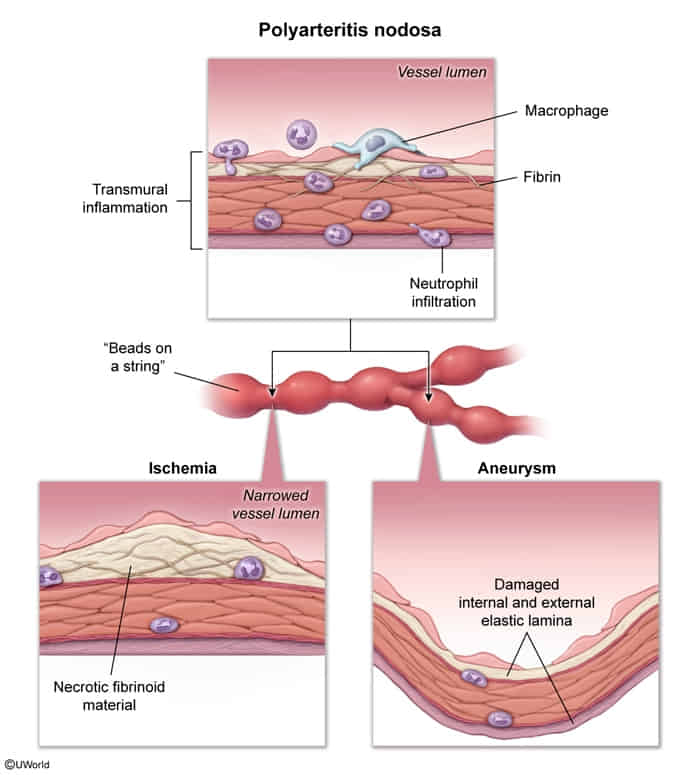
- Transmural inflammation of the arterial wall with fibrinoid necrosis
Pathophysiology
Clinical features
- Constitutional: Fever, weight loss, malaise, headache.
- Renal: Renal artery involvement leads to renal ischemia and activation of RAAS Hypertension.
- Note: No glomerulonephritis (urine is typically free of RBC casts).
- Gastrointestinal: Abdominal pain (“intestinal angina”), melena, nausea (due to mesenteric arteritis).
- Neurologic: Mononeuritis multiplex (asymmetric motor/sensory deficit, e.g., wrist drop).
- Dermatologic: Livedo reticularis, subcutaneous nodules, palpable purpura.
- Usually spares the lungs
- Unlike GPA
Mnemonic
In PAN, the Pulmonary Artery is Not involved, PANmural inflammation of the arterial wall is present, and PAN may be associated with hePAtitis B.
Tip
PAN should be considered in adults < 65 years of age presenting with stroke or myocardial infarction.
Diagnostics
Biopsy
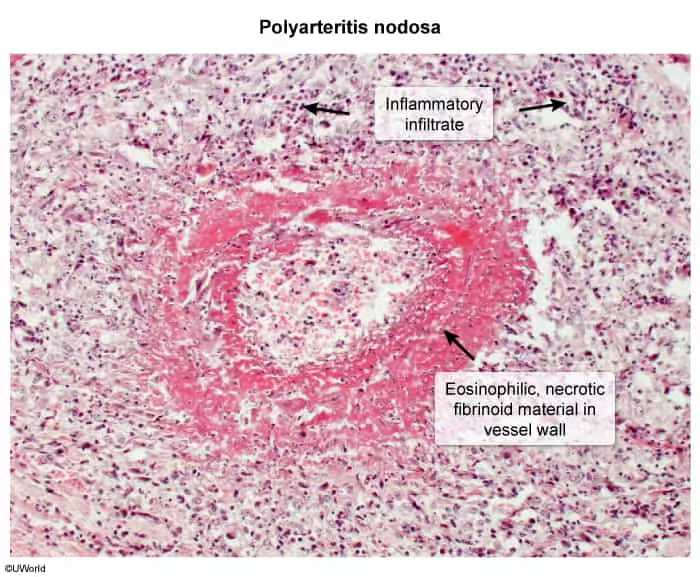
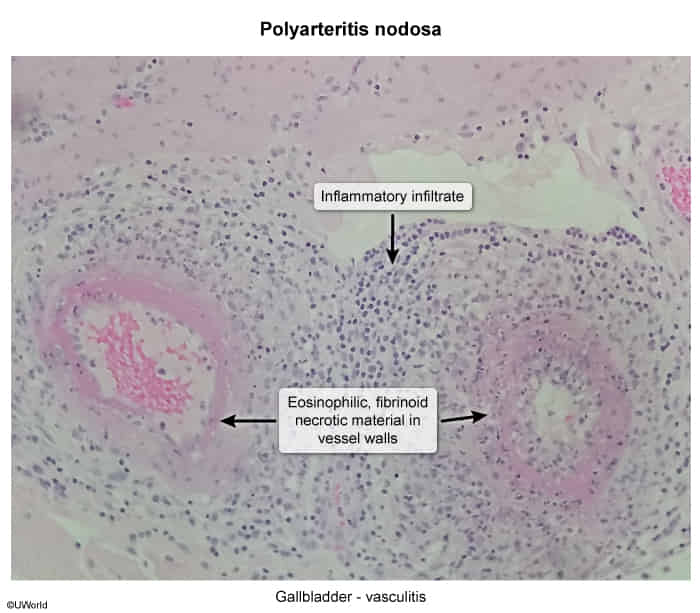
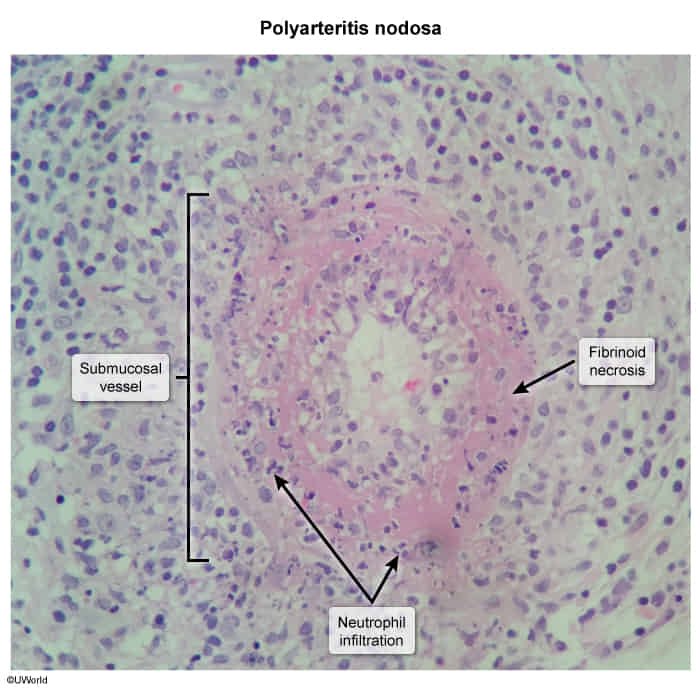
- Transmural inflammation with leukocytic infiltration and fibrinoid necrosis
- Inflammatory lesions in various stages of development and regeneration
Visceral angiography
- Findings: most commonly seen in the renal, mesenteric, and hepatic artery branches (pulmonary arteries are usually not affected)
- Numerous microaneurysms (1–5 mm in diameter)
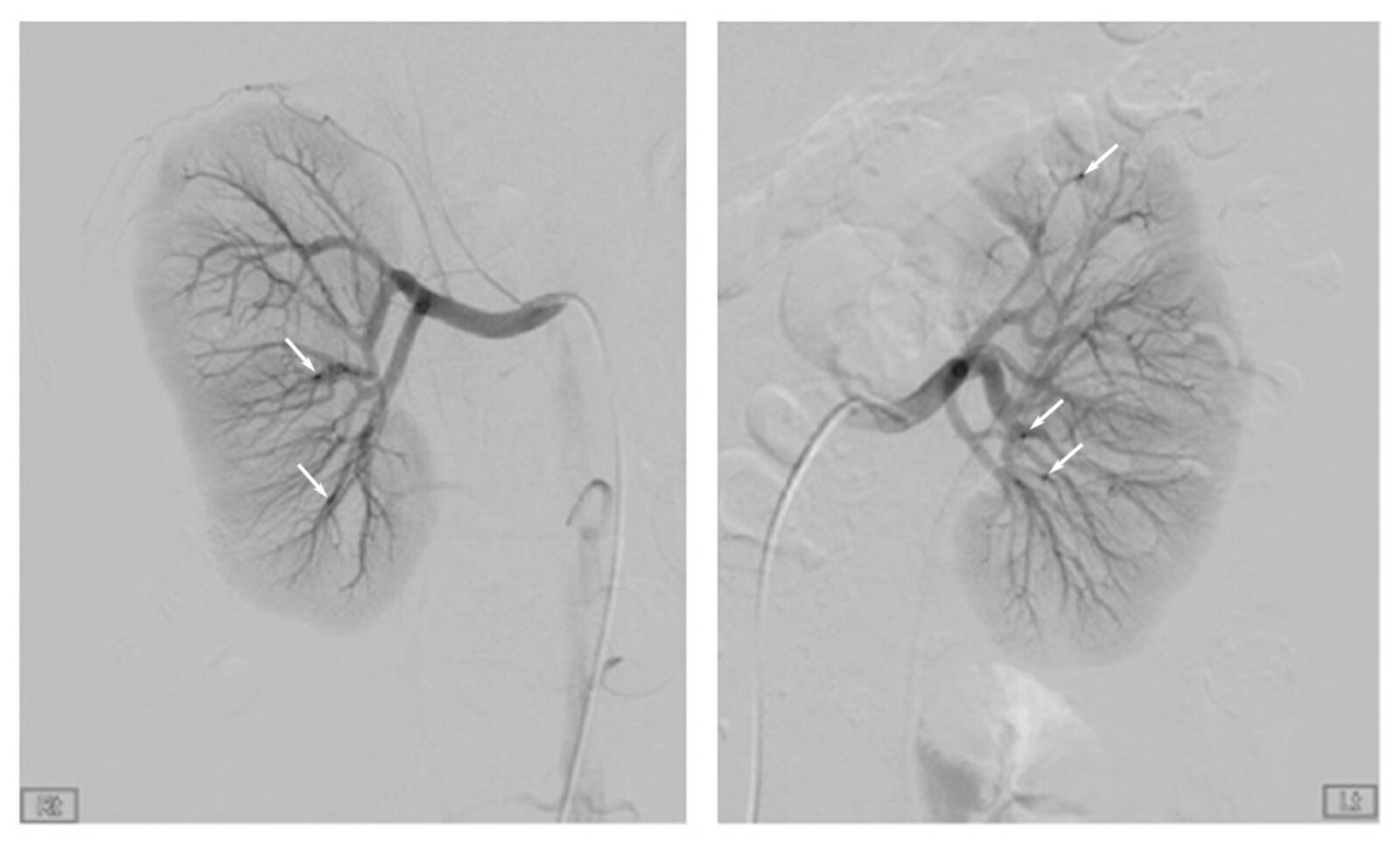
- Stenosis of small muscular arteries and medium-sized vessels
- Numerous microaneurysms (1–5 mm in diameter)