Programmed, ATP-dependent cell death of single cells or small groups, crucial for development and tissue homeostasis. It can be physiologic (e.g., embryogenesis, endometrial shedding) or pathologic (e.g., cell death in tumors, viral hepatitis). It is generally not associated with inflammation.
Key Pathways
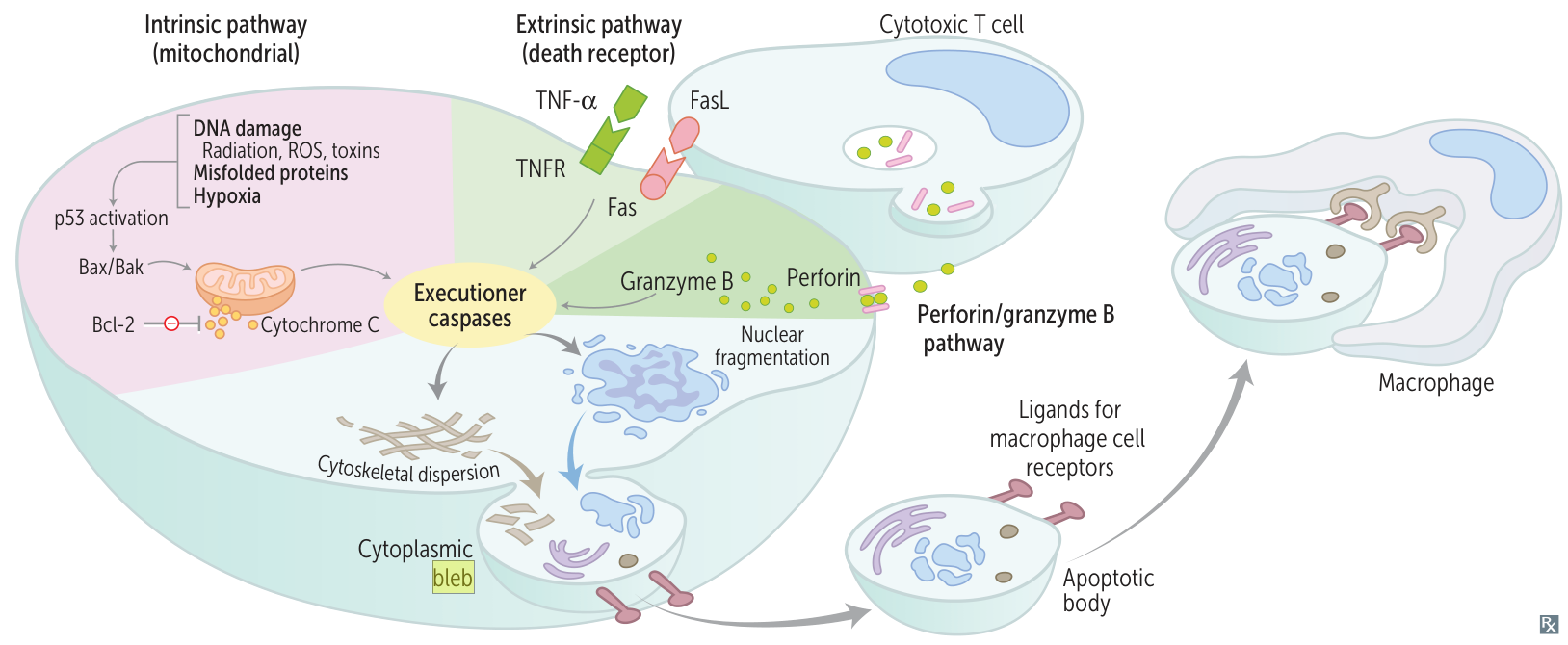
Intrinsic (Mitochondrial) Pathway: Triggered by cellular stress (e.g., DNA damage, growth factor withdrawal). Regulated by the Bcl-2 family of proteins. Pro-apoptotic proteins (e.g., Bax, Bak) create pores in the mitochondrial membrane, releasing cytochrome c. Cytochrome c activates caspase-9, the initiator caspase.
Extrinsic (Death Receptor) Pathway: Initiated by external signals. Fas ligand (FasL) on cytotoxic T-cells binds to the Fas receptor (CD95) on the target cell, or TNF-α binds to its receptor. This activates caspase-8, the initiator caspase.
Common Pathway: Both pathways converge to activate executioner caspases like caspase-3, which dismantle the cell.
Morphology
Cell shrinkage, chromatin condensation (pyknosis), and formation of apoptotic bodies. The cell membrane remains intact. Apoptotic bodies are phagocytosed by macrophages.
Necrosis
Pathophysiology/Etiology
Uncontrolled cell death of large groups of cells following exogenous injury (e.g., ischemia, infection). It is always a pathologic process and incites an inflammatory response due to the loss of membrane integrity and leakage of cellular contents.
Types of Necrosis
Coagulative: Most common type, often due to ischemia in solid organs (except the brain), like the heart or kidney. Histology shows preserved cell outlines with loss of nuclei and eosinophilic cytoplasm.
Liquefactive: Seen in bacterial abscesses and brain infarcts. Tissue is digested by hydrolytic enzymes, forming a viscous liquid (“pus”).
Caseous: A combination of coagulative and liquefactive necrosis, classically seen in tuberculosis (TB). Appears “cheese-like” on gross examination.
Fat: Occurs in acute pancreatitis and breast trauma. Damaged cells release lipases, which break down triglycerides into fatty acids that saponify with calcium, creating chalky-white deposits. t
Fibrinoid: Seen in blood vessel walls during vasculitis or malignant hypertension. Characterized by immune complex deposition and fibrin, resulting in a bright pink, amorphous appearance on H&E stain.
Gangrenous: A clinical term describing ischemic necrosis of a limb, often with a superimposed bacterial infection (wet gangrene).
Fibrinoid necrosis
Definition: a type of necrosis characterized by small blood vessel injury with accumulation of fibrin and other plasma proteins.
Pathophysiology: vessel wall damage caused by immune complex deposition (e.g., due to type III hypersensitivity reaction) → fragmentation of collagenous and elastic fibers → leakage of fibrin and other plasma proteins
Microscopic appearance
Visible damage: thick walls with fragments of embedded cellular debris, serum, and fibrin
A programmed, “necrosis-like” cell death that is caspase-independent. It is triggered by factors like TNF-α and involves RIPK1, RIPK3, and MLKL proteins, leading to inflammation. Serves as a backup mechanism when apoptosis is inhibited.
Pyroptosis
An inflammatory form of programmed cell death triggered by intracellular pathogens. It involves the activation of caspase-1 (via the inflammasome), which cleaves gasdermin D to form membrane pores. This leads to cell lysis and the release of pro-inflammatory cytokines like IL-1β and IL-18, causing fever.
Autophagy
A cellular “self-eating” process where cytoplasmic components are delivered to lysosomes for degradation. It’s a survival mechanism during nutrient deprivation but can also be involved in cell death.