Common causes
- Proximal injury: supracondylar fracture of humerus
- Distal injury
- Carpal tunnel compression
- Wrist laceration (suicide attempt)
- Pronator teres syndrome: compression of the median nerve between the humeral and ulnar heads of the pronator teres
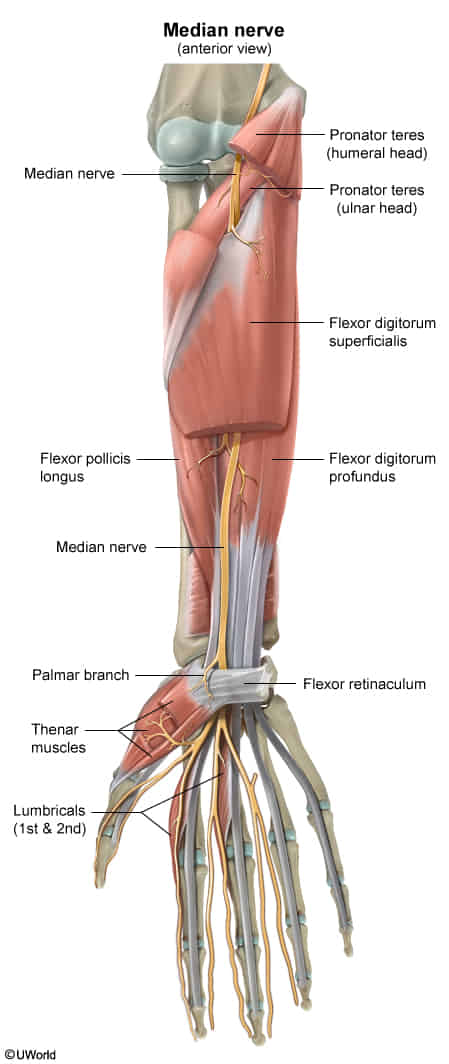
Motor deficits
- The key is whether flexor digitorum profundus is damaged.
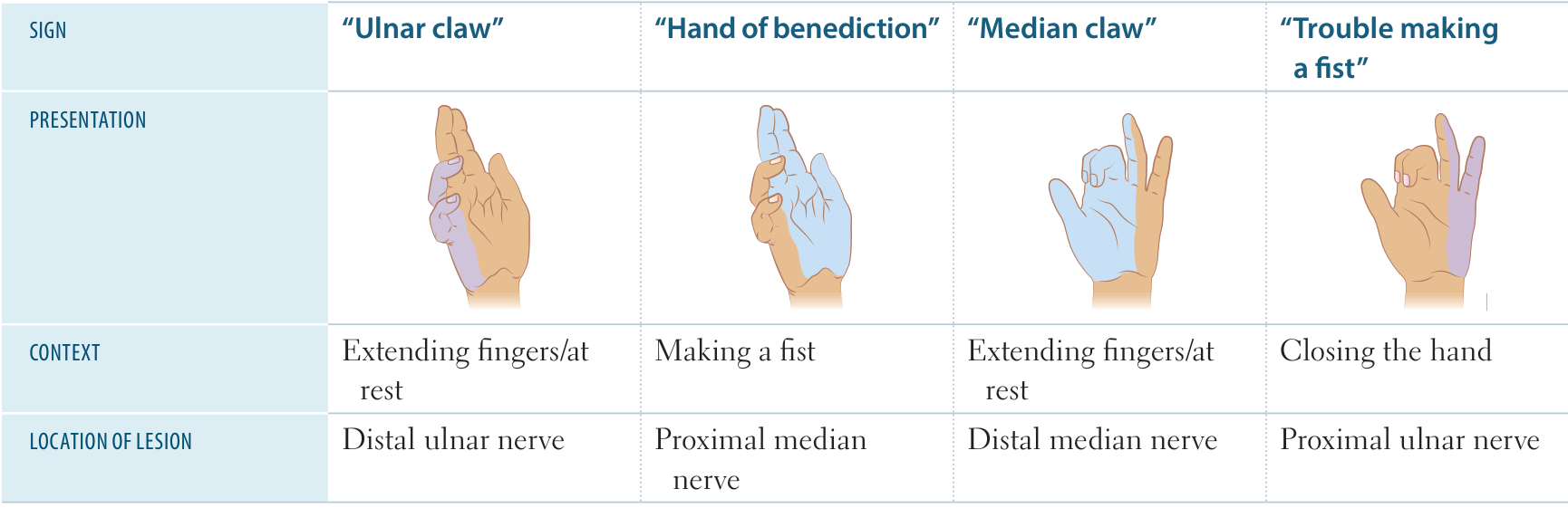
- Nerves controlling flexor digitorum profundus branches out below the elbow. So it’s spared in distal lesion, but included in proximal lesion. So the claw hand is more prominent in distal lesion.
- Anterior Interosseous Nerve → flexor digitorum profundus → flexion of index and middle finger
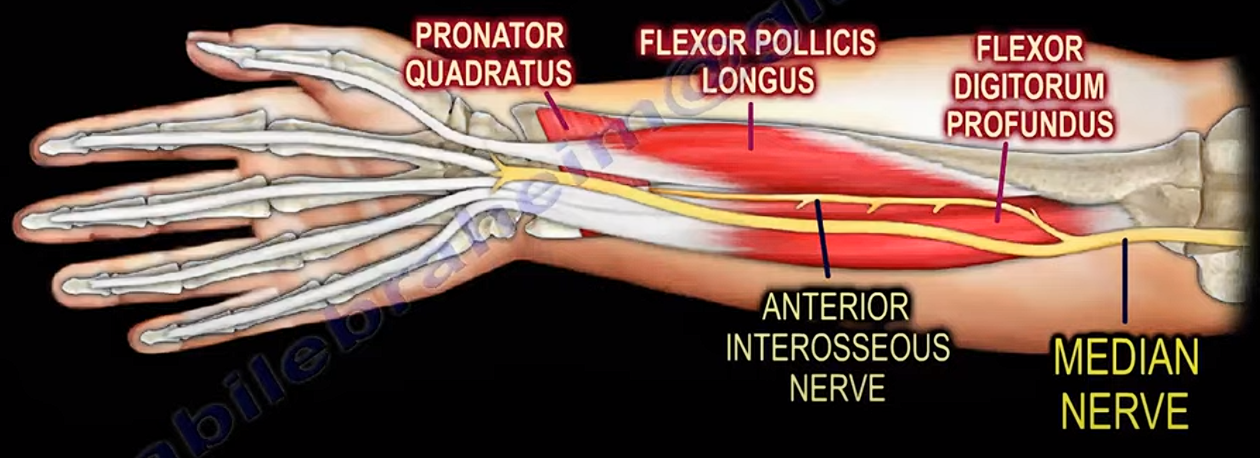
- Flexor digitorum profundus
- has dual innervation: the medial part is supplied by ulnar nerve
- Controls wrist, MCP, and DIP joints: flexion
- Flexor digitorum profundus
- Flexor digitorum superficialis
- Controls wrist, MCP, and PIP joints: flexion
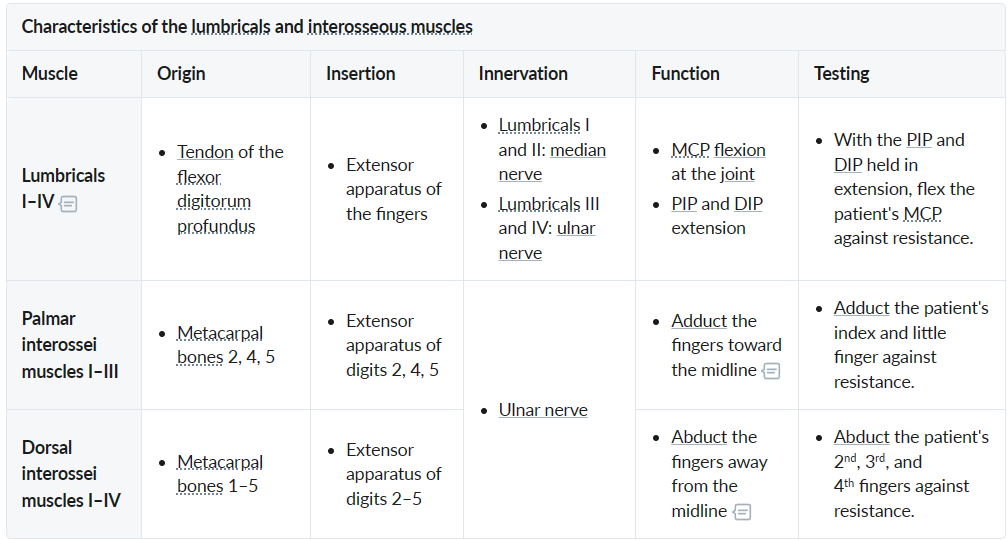
- Lumbricals and interossei
- Ape hand: inability to oppose and abduct the thumb due to injury of the proximal or distal median nerves impairing the thenar muscles’ functions
Carpal tunnel syndrome
- Results from a lesion that reduces the size of the carpal tunnel (fluid retention, infection, dislocation of lunate bone)
- Median nerve – most sensitive structure in the carpal tunnel and is the most affected
- Risk factors
- Manual work: increased risk in workers using vibrating tools or prolonged, forceful, and repetitive flexion/extension of the wrist
- Rheumatoid arthritis, Osteoarthritis
- Pregnancy (edema) t
- Systemic amyloidosis
- Renal failure and dialysis-associated deposition of amyloid
- Deposition of beta-2 microglobulin (dialysis-associated amyloidosis) in the carpal tunnel (injection site)
- Diabetes mellitus
- Hypothyroidism
- Clinical manifestations:
- Pins and needles or anesthesia of the lateral 3.5 digits
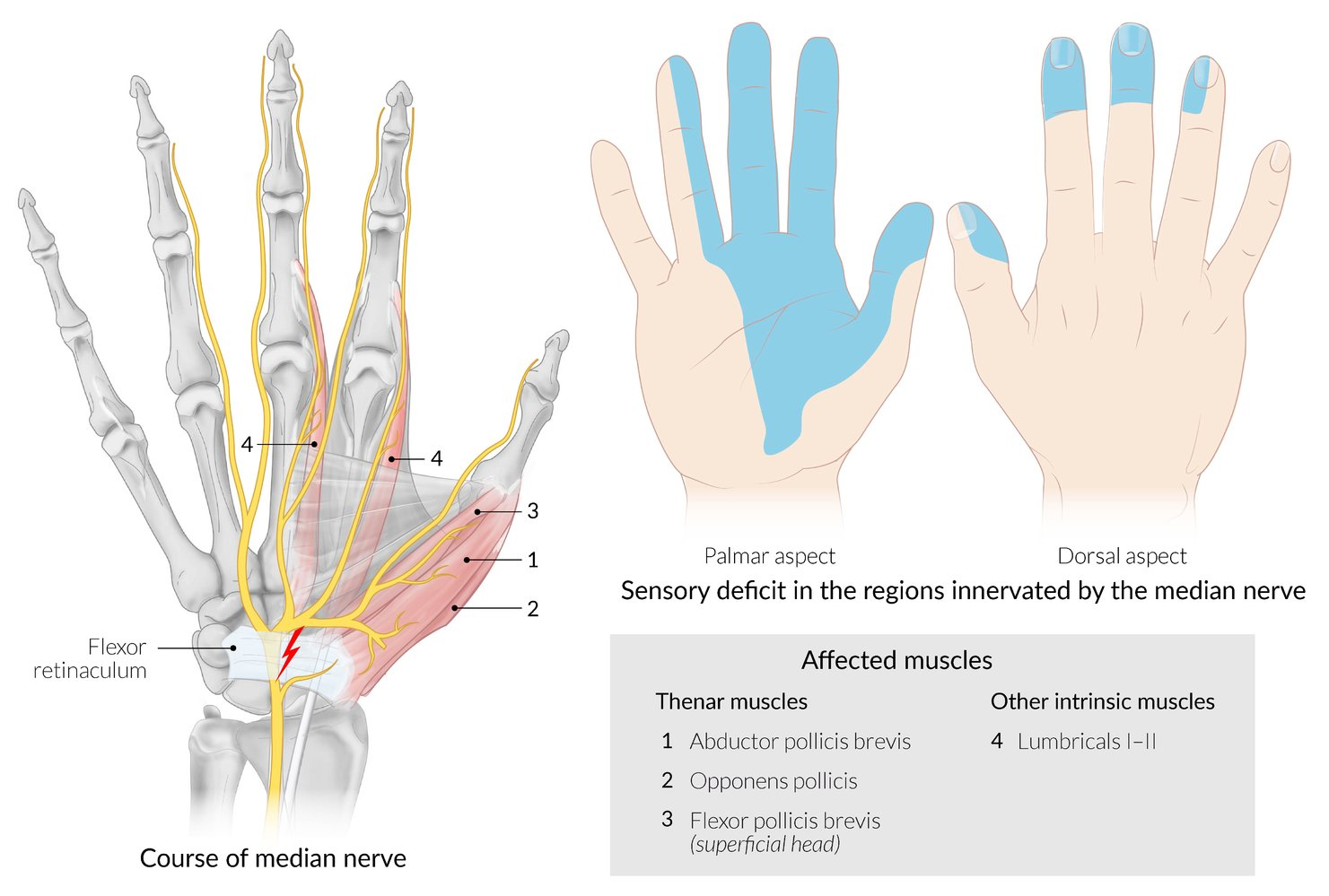
- Palm sensation is not affected because superficial palmar cutaneous branch passes superficially to carpal tunnel
- Similar situation in Guyon canal syndrome
- Ape hand deformity - absent of OPPOSITION
- Nocturnal Sx: Pain often wakes pt at night; shaking hands relieves Sx (“flick sign”). t
- Night Sx: Wrist flexion during sleep + supine fluid redistribution intracarpal pressure median nerve ischemia.
- Flick Sign: Restores arterial perfusion + venous congestion.
- Pins and needles or anesthesia of the lateral 3.5 digits
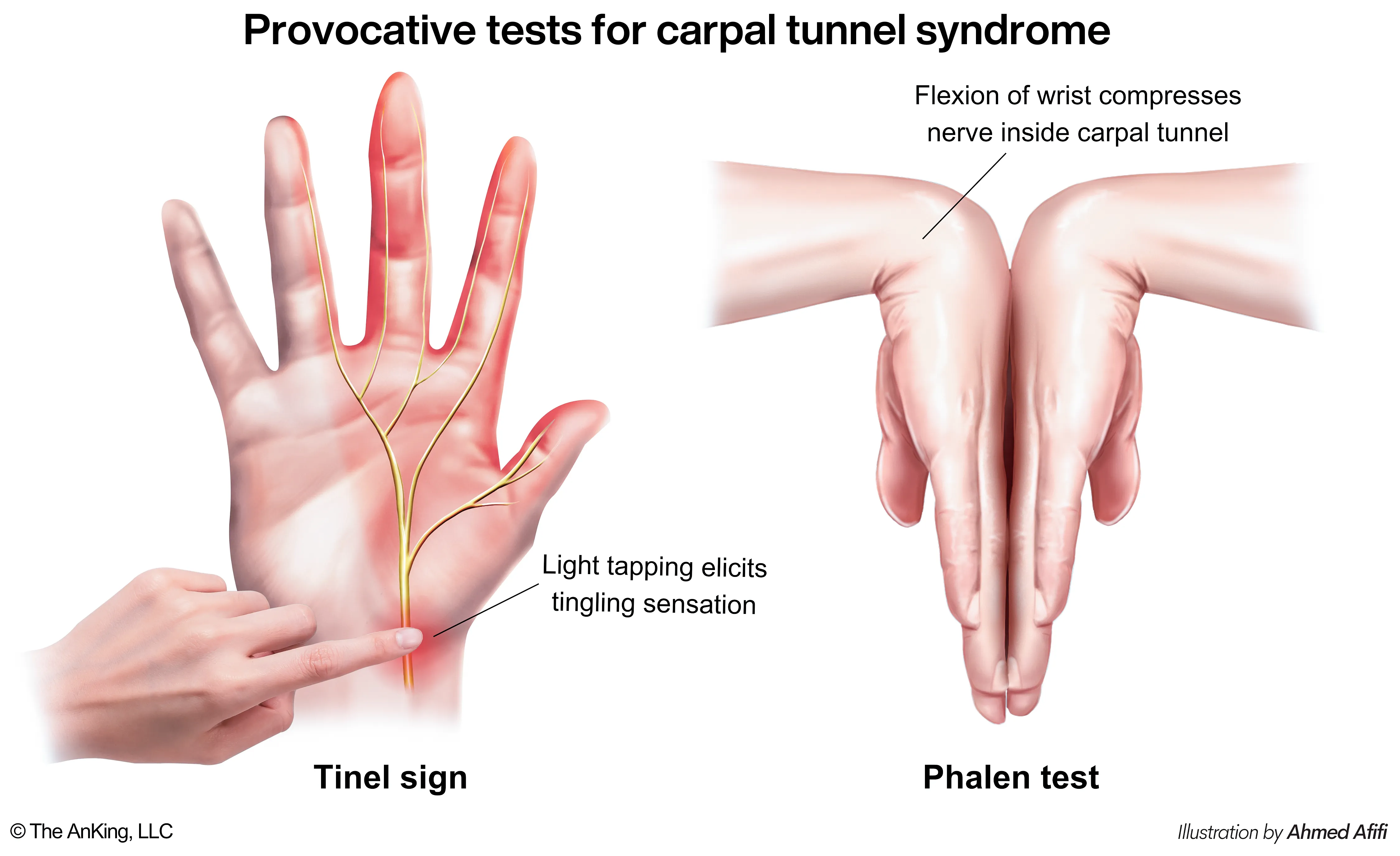
- Diagnostics / Physical Exam
- Phalen maneuver: Flexing wrists for 60 sec reproduces paresthesia.
- Tinel sign: Tapping over the carpal tunnel elicits tingling.
- Nerve Conduction Studies (NCS): Gold standard for confirmation. Shows ↓ conduction velocity and ↑ latency across the wrist.