Intrauterine risk factors: infants born to mothers with diabetes
Pathophysiology
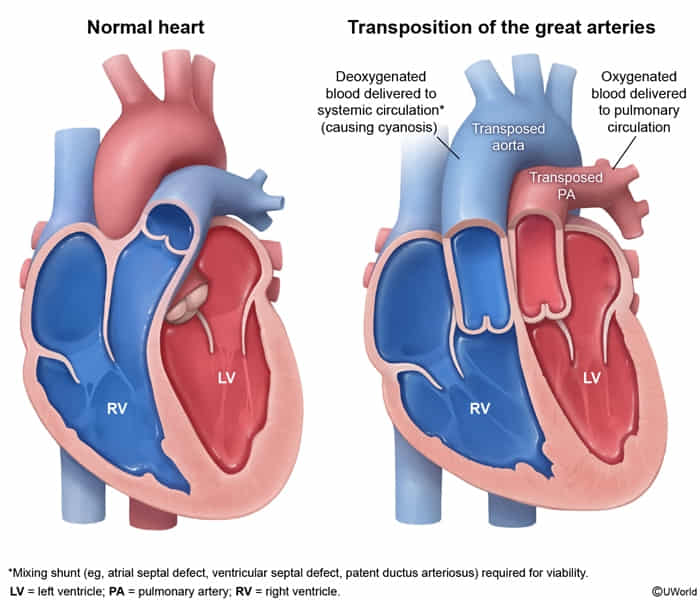
Failed spiralingt of the aorticopulmonary septum → RV emptying into the aorta and LV into the pulmonary artery → complete isolation of the pulmonary and systemic circuits → ↓ oxygenated blood entering the systemic circulation
Fatal, unless mixing occurs via an intracardiac shunt (e.g., PFO, VSD, ASD) or via an extracardiac connection (e.g., PDA)
Clinical features
Cyanosis: Severe, progressive cyanosis within hours of birth. Not responsive to supplemental O2 (Hyperoxic test negative).
PE: Single S2 (aorta is anterior and closer to chest wall, PA is posterior). c
Normally the PA is anterior, P2 is normally audible (though softer than A2).
Murmur: Usually absent. If present, suggests associated VSD or PS.
Tachypnea: Quiet tachypnea (no increased work of breathing initially).
Diagnostics
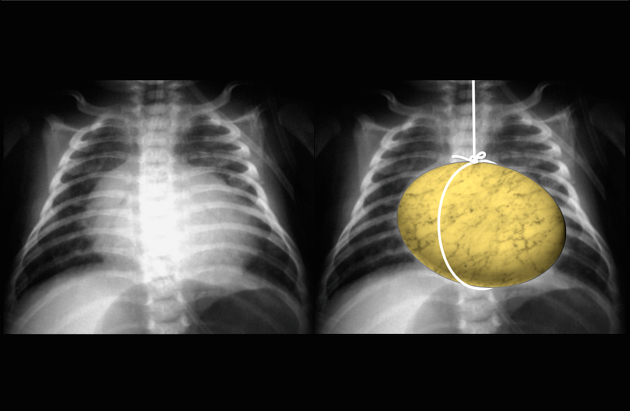
Chest x-ray: narrow mediastinum ± cardiomegaly (“egg on a string”)
This anterior-posterior alignment (rather than the normal side-by-side/wrapping relationship) creates the narrow mediastinum (“egg-on-a-string”).
The string represents the narrow superior mediastinum due to stress-induced thymic atrophy and hyperinflated lungs.
Hyperoxia test: little to no ↑ in arterial oxygenation with 100% O2