Etiology
The most common form of congenital LQTS (LQTS type 1) is caused by a defect in the slow delayed rectifier voltage-gated potassium channel.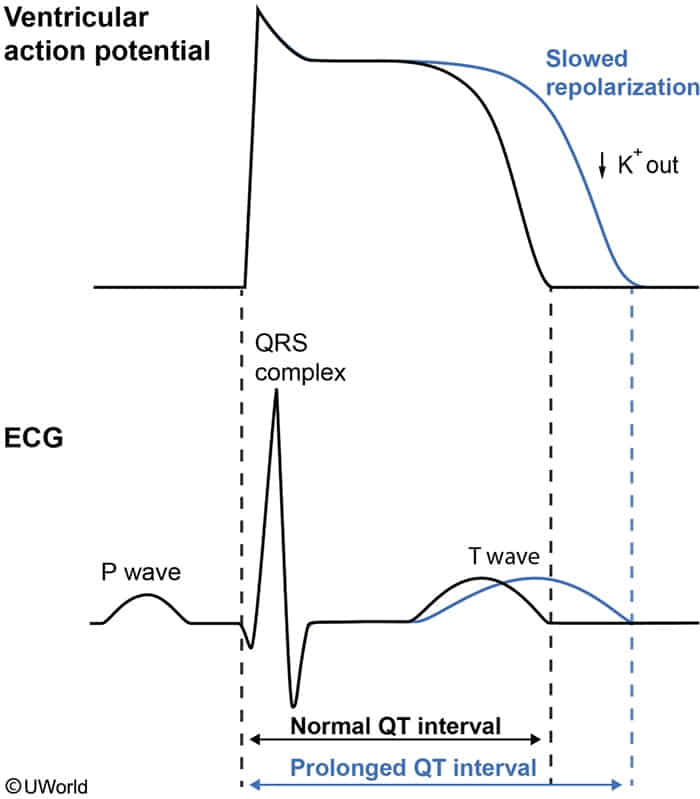
Acquired LQTS
A prolonged QT interval indicates delayed ventricular de- or repolarization, most commonly caused by drugs (mainly via inhibition of potassium efflux) or electrolyte imbalances.
- Drug-induced LQTS: Usually substances that block potassium outflow during the rapid repolarization phase
- Macrolides & fluoroquinolones
- Antiemetics (eg, ondansetron)
- Azoles (eg, fluconazole)
- Antipsychotics (Haloperidol, Quetiapine, Ziprasidone), TCAs & SSRIs c
- Some opioids (eg, methadone, oxycodone) t
- Class Ia antiarrhythmics (eg, quinidine)
- Class III antiarrhythmics (eg, dofetilide, sotalol, amiodarone)
- Despite prolonging the QT interval, Amiodarone rarely causes Torsades de Pointes (TdP). t
- Electrolyte imbalances: hypokalemia, hypomagnesemia, hypocalcemia
- Hypokalemia: Inhibits the IKr (rapid delayed rectifier K+) current. Slows Phase 3 (repolarization) by reducing K+ efflux.
- Hypomagnesemia: Directly inhibits K+ channels (like IKr) and promotes renal K+ wasting, often causing concurrent hypokalemia. Slows Phase 3 (repolarization).
- Hypocalcemia: Delays inactivation of L-type Ca2+ channels. Prolongs Phase 2 (plateau) of the action potential.
- Endocrine disorders: hypothyroidism
Clinical features
“Pure” LQTS is purely an electrical phenotype. The clinical features only manifest when that underlying electrical vulnerability degrades into a hemodynamically unstable arrhythmia (specifically TdP or VF).
- Presentation ranges from asymptomatic to recurrent palpitations, dizziness, or syncope. c
- Triggers: Exertion/swimming (LQT1), sudden loud noises/alarms (LQT2), sleep/rest (LQT3).
- Can present as seizure-like activity (due to cerebral hypoperfusion from dysrhythmia) or Sudden Cardiac Death (SCD).
Diagnosis
- Initial/Screening: 12-lead ECG. QTc > 440 ms (males) (2 big blocks) or > 460 ms (females). QTc > 500 ms carries high risk for Torsades de Pointes (TdP). Broad, altered, or notched T waves may be seen.
- Key Labs: Serum electrolytes (K, Mg, Ca) to rule out acquired causes.
- Confirmatory/Gold Standard: Genetic testing (for congenital forms, identifies specific channelopathies like KCNQ1, KCNH2). Audiometry (to screen for Jervell and Lange-Nielsen).
Complications
- Ventricular tachycardia (torsades de pointes)
- Ventricular fibrillation
- Asystole
- Sudden cardiac death