Description: a rare type of hepatic encephalopathy aspirin use for viral illness in children < 19 years
Etiology: aspirin use in individuals < 19 years of age with a febrile illness
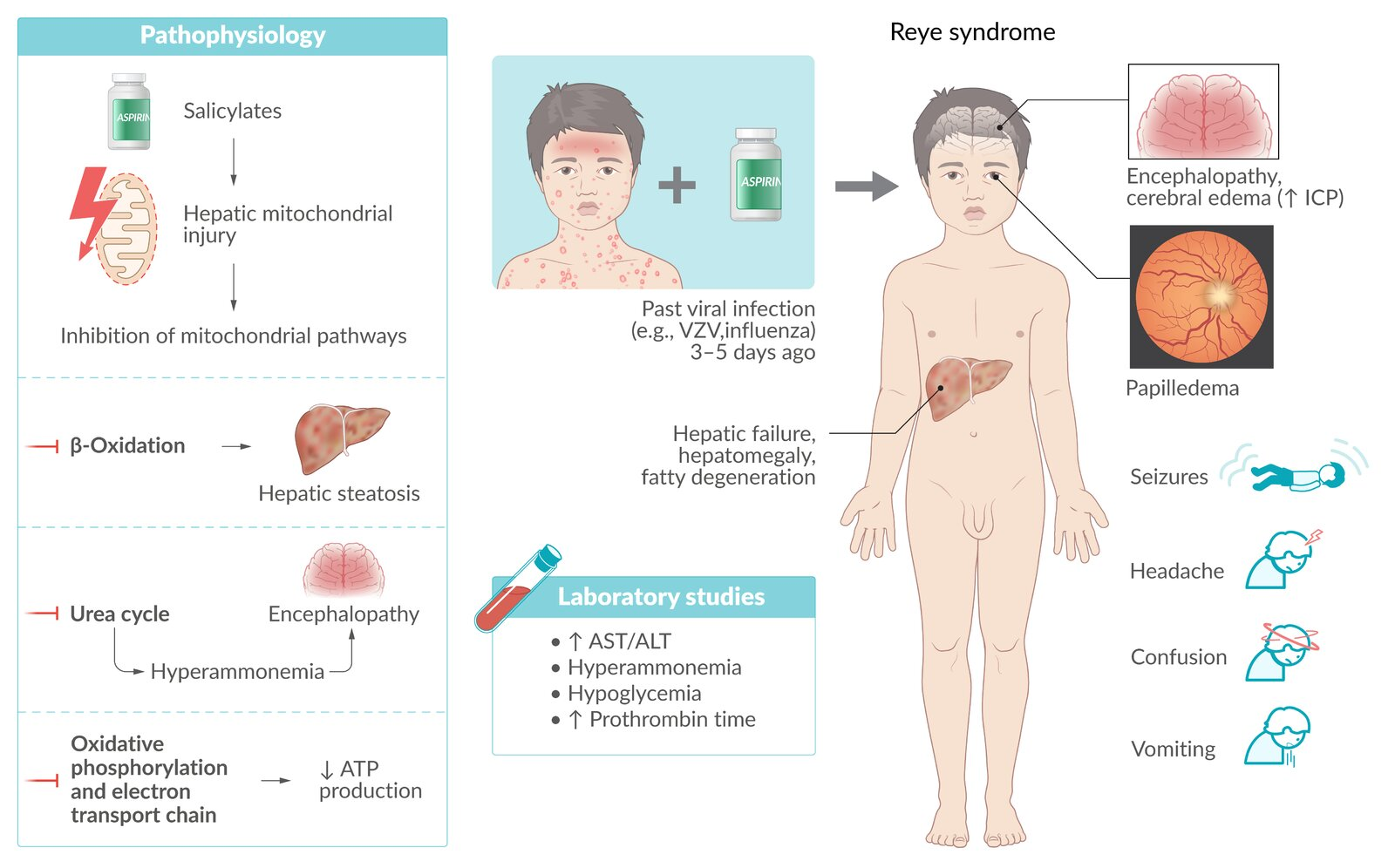
Pathophysiology
Aspirin use in children during viral infection (eg, influenza , varicella)
Mitochondrial toxicity → impaired fatty acid metabolism
Microvesicular fat deposits in the liver Hepatic dysfunction → hyperammonemia
Diffuse astrocyte swelling (ie, cerebral edema)
Clinical features
Preceding viral infection (e.g., influenza , varicella or viral gastroenteritis): The first symptoms of Reye syndrome usually begin 3–5 days after a viral illness.
Acute encephalopathy
Severe vomiting Altered mental status (ranging from lethargy to delirium and coma) Neurological symptoms (e.g., seizures , fixed pupils)
Liver failure
Prevention
Aspirin should be avoided in individuals < 19 years of age, especially those with fever.
Exception: children with Kawasaki disease
Differential diagnostics
t
Feature Salicylate (ASA) Acetaminophen (APAP) Reye Syndrome Path Uncouple oxidative phosphorylation (leads to hyperthermia); Direct stimulation of resp center.Glutathione depletion → NAPQI → Mito dysfunction (↓ β → Microvesicular fatty change in liver Hx/Trigger OD; Wintergreen oil OD (esp. w/ CYP inducers/EtOH) Child + Virus + ASA Key Sx Tinnitus , Hyperthermia, TachypneaRUQ pain, Fulminant liver failure Encephalopathy, Vomiting Labs/Path Mixed Resp Alk + Met AcidosisZone 3 Necrosis , ↑↑ Microvesicular fatty liver , ↓ ↑ Tx NaHCO3 (Alkalinize urine), DialysisN-acetylcysteine (restore glutathione)Supportive
Link to original