Epidemiology
Leading cause of acute liver failure
Etiology
Pathophysiology
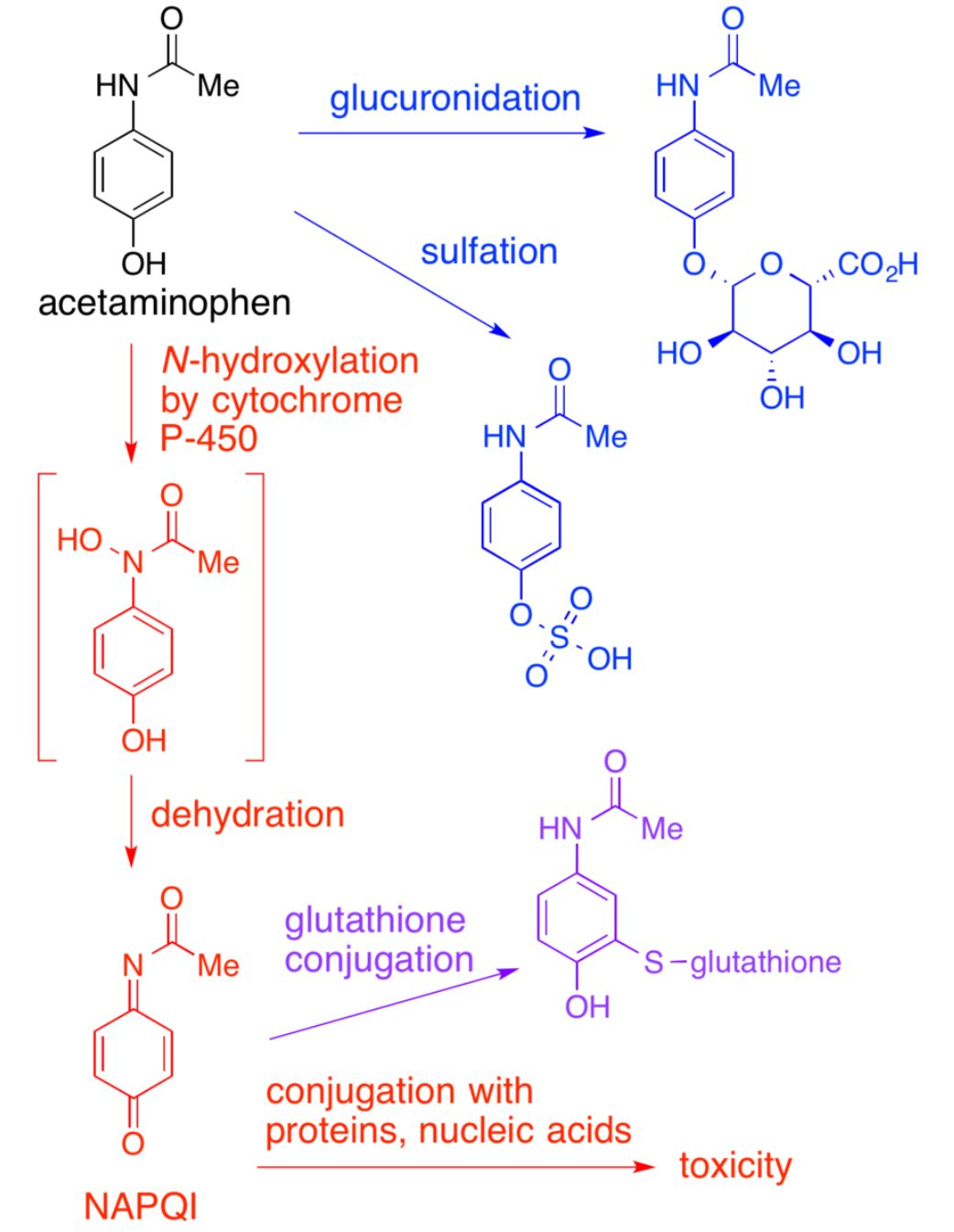
- Exhaustion of hepatic metabolic pathways causes accumulation of a toxic metabolite of acetaminophen, N-acetyl-p-benzoquinoneimine (NAPQI).
- Glutathione initially inactivates NAPQI, but its reserves are eventually depleted, leading to NAPQI accumulation.
- NAPQI → irreversible oxidative hepatocyte injury → liver cell necrosis
- APAP-induced hepatotoxicity
- Defined as peak AST or ALT > 1000 IU/L
- Most commonly caused by APAP overdose
- Occurs rarely at therapeutic doses in patients with:
- Alcohol consumption
- Prolonged fasting
- Chronic liver disease
Clinical features
- Nausea, vomiting
- Pallor
- RUQ pain
- Signs of acute liver failure
Diagnostics
Differential diagnostics
| Feature | Salicylate (ASA) | Acetaminophen (APAP) | Reye Syndrome |
|---|---|---|---|
| Path | Uncouple oxidative phosphorylation (leads to hyperthermia); Direct stimulation of resp center. | Glutathione depletion NAPQI centrilobular hepatic necrosis. | Mito dysfunction ( -oxidation) Microvesicular fatty change in liver |
| Hx/Trigger | OD; Wintergreen oil | OD (esp. w/ CYP inducers/EtOH) | Child + Virus + ASA |
| Key Sx | Tinnitus, Hyperthermia, Tachypnea | RUQ pain, Fulminant liver failure | Encephalopathy, Vomiting |
| Labs/Path | Mixed Resp Alk + Met Acidosis | Zone 3 Necrosis, AST/ALT | Microvesicular fatty liver, Glucose, Ammonia |
| Tx | NaHCO3 (Alkalinize urine), Dialysis | N-acetylcysteine (restore glutathione) | Supportive |
Treatment
- Antidote: PO or IV N-acetylcysteine (NAC) is used to treat and prevent APAP-induced hepatoxicity.
- NAC regenerates glutathione