Associated with Thymoma.
Pathophysiology
Thymus involvement
- Muscle-like (myoid) cells in the thymus express AChR → autoreactive targeting by T cells → production of acetylcholine receptor antibodies (AChR antibodies)
Acetylcholine receptor antibodies
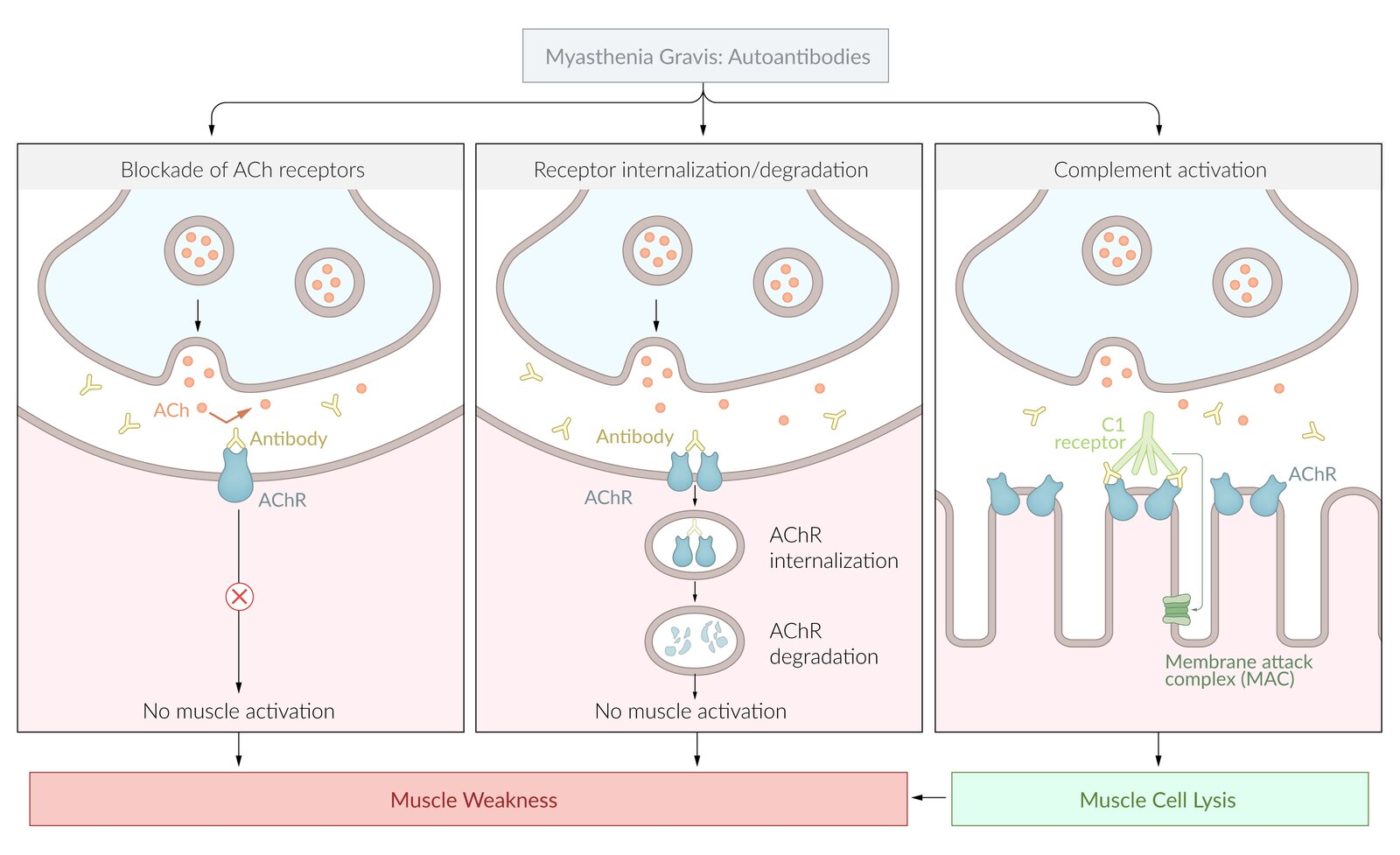
- Responsible for inhibition of signal transduction at the neuromuscular junction (NMJ)
- Antibodies target postsynaptic AChRs of normal muscle cells → competitive inhibition of acetylcholine (ACh) → AChR decay through receptor internalization (↓ receptor density at the postsynaptic membrane) and activation of complement (→ muscle cell lysis) → impaired signal transduction at the NMJ → skeletal muscle weakness and fatigue
- Seropositive MG (80–90% of cases): positive assays for antibodies (in blood) against the acetylcholine receptor (AChR-Ab)
- Seronegative MG (10–20% of cases): negative for AChR antibodies, but may be positive for muscle-specific tyrosine kinase antibodies (MuSK antibodies)
Diagnostics
- Initial test: anti-AChR antibodies (highly specific for MG)
Warning
Because MG and LEMS are neuromuscular junction disorders, muscle biopsy of these conditions will be normal. Unlike in myopathies (e.g. Polymyositis, Dermatomyositis, Mitochondrial myopathies)
Intracellular Microelectrode Recordings t
- MEPP (Miniature End-Plate Potential): Small depolarization caused by the spontaneous release of a single vesicle (quantum) of ACh.
- Significance: Amplitude reflects Postsynaptic receptor sensitivity/density.
- EPP (End-Plate Potential): Summation of potentials caused by massive ACh release after a nerve impulse.
- Significance: Determines if threshold is reached to trigger muscle action potential.
- Quantal Content: The number of vesicles released per nerve impulse.
- Significance: Reflects Presynaptic function.
| Disease | Defect Location | MEPP Amplitude (Postsynaptic Sensitivity) | Quantal Content (Presynaptic Release) | EPP Amplitude | Repetitive Nerve Stimulation |
|---|---|---|---|---|---|
| Myasthenia Gravis | Postsynaptic (ACh Receptor) | ↓ Decreased | Normal | ↓ Decreased | Decremental (Worsens with use) |
| Lambert-Eaton | Presynaptic (VG-Ca²⁺ Channel) | Normal | ↓ Decreased | ↓ Decreased | Incremental (Improves with use) |
| Botulism | Presynaptic (SNARE proteins) | Normal | ↓↓ Decreased | ↓↓ Decreased | Incremental* (May improve at high Hz) |
Differential diagnostics
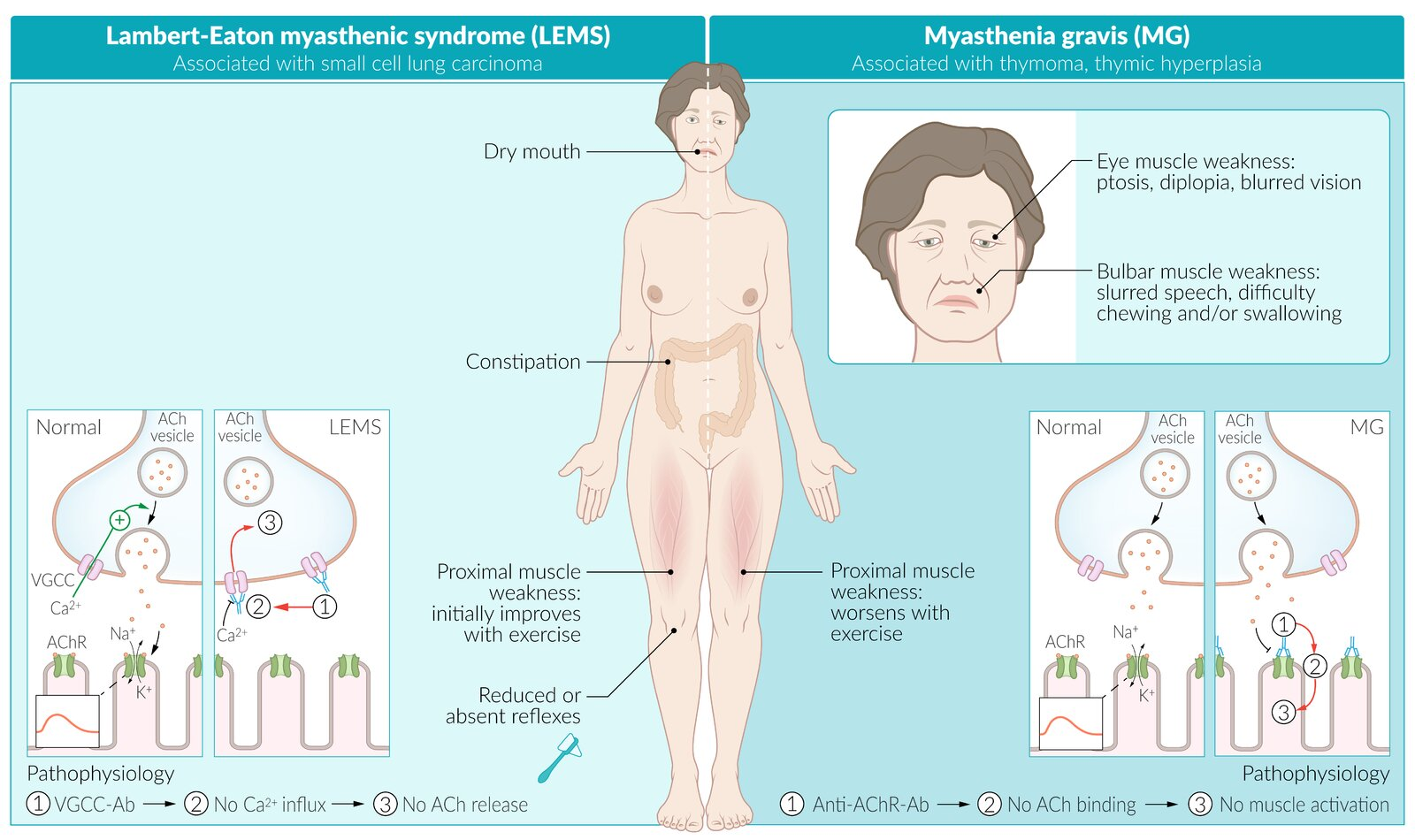
Lambert-Eaton myasthenic syndrome (LEMS)
- Etiology
- Paraneoplastic: associated with small-cell lung carcinoma (in ⅔ of patients with LEMS)
- Pathophysiology: autoantibodies directed against presynaptic voltage-gated calcium channels (anti-VGCC antibodies) → ↓ Ca2+ influx → ↓ presynaptic vesicle fusion → impaired acetylcholine release in the NMJ
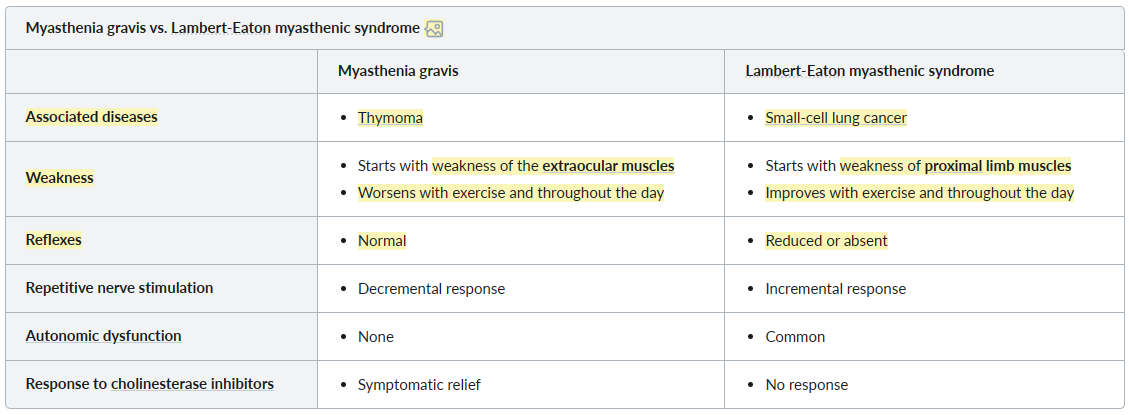
| Feature | Myasthenia Gravis (MG) | Lambert-Eaton (LEMS) |
|---|---|---|
| Pathophysiology | Post-synaptic: Anti-AChR Ab. | Pre-synaptic: Anti-VGCC Ab. |
| Hallmark Sx | Weakness worsens with use/fatigue. | Strength improves with repetition. |
| Initial Presentation | Eyes/Face (ptosis, diplopia). | Proximal legs (trouble rising). |
| Deep Tendon Reflexes | Normal. | ↓ or Absent. |
| Autonomic Sx | Rare. | Common (dry mouth, impotence). |
| Association | Thymoma / Thymic hyperplasia. | Small Cell Lung Cancer. |
| EMG (RNS) | Decremental response. | Incremental response. |
Tip
- Extraocular muscles: move frequently, so they are first affected.
- MG: Repeated nerve stimulation → decreasing ACh release (as the storage is limited) → worsen symptoms
- LEMS: More depolarization → more ACh release → improved symptoms
Treatment
- Symptomatic Tx: Acetylcholinesterase inhibitors (e.g., Pyridostigmine) are first-line to increase ACh availability at the NMJ.
- Immunosuppression: Chronic oral corticosteroids (e.g., prednisone) are often used for long-term management. Steroid-sparing agents like azathioprine or mycophenolate mofetil can also be utilized.
- Thymectomy: Recommended for all patients with a thymoma. It is also considered for many patients with generalized AChR-positive MG, as it can be curative or lead to clinical improvement.
- Acute Crisis Mgmt: For myasthenic crisis, treatment involves plasmapheresis or IVIG for rapid effect, along with respiratory support (e.g., mechanical ventilation).