Transmission is via direct person-to-person contact
Pathophysiology
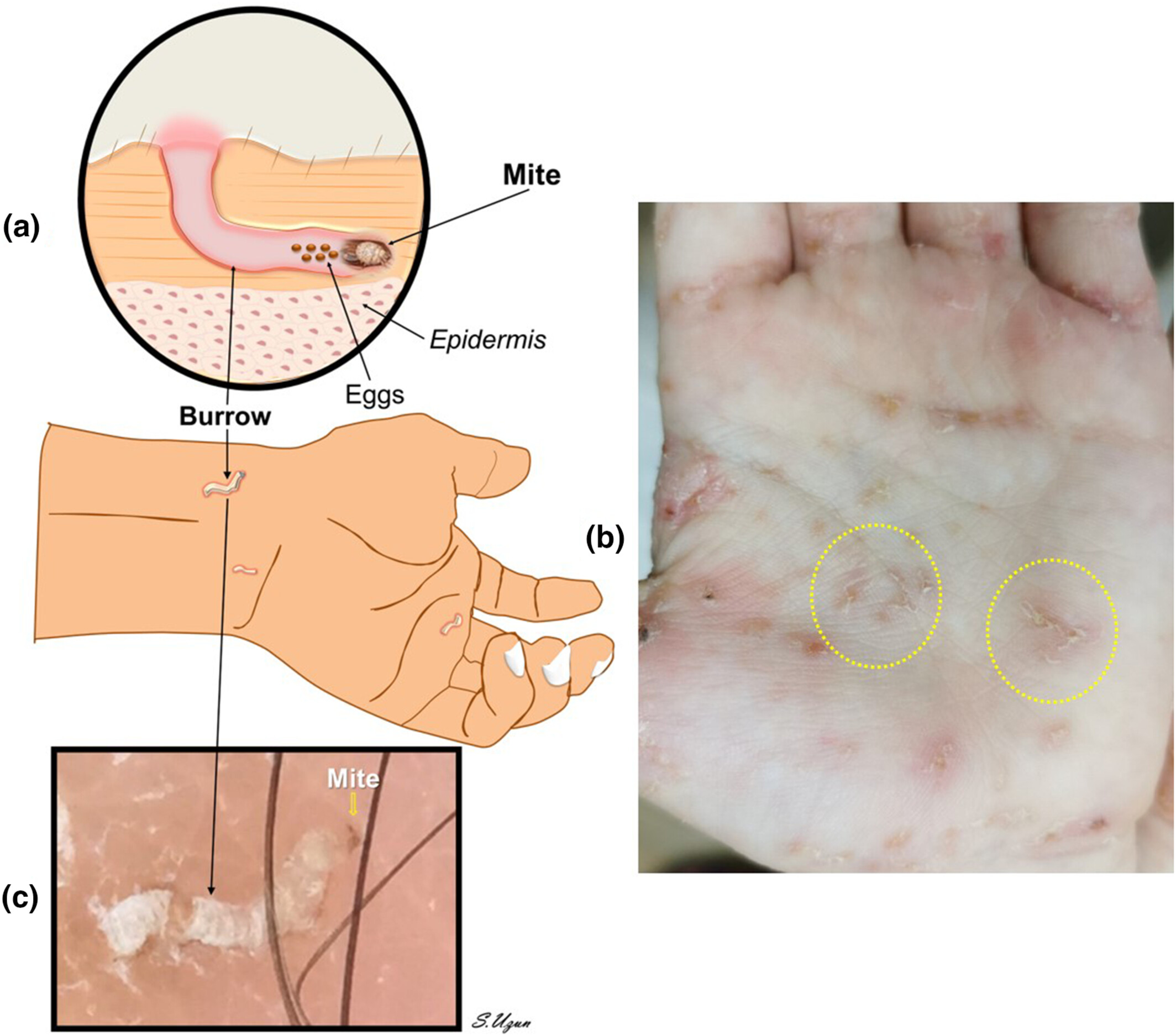
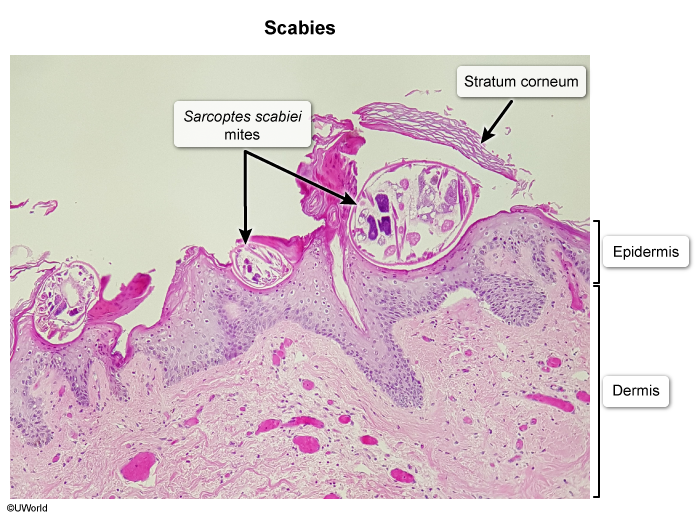
The fertilized, female mite tunnels into the superficial skin layer (stratum corneum), forming burrows in which she lays her eggs and deposits feces (scybala).
After 2 months, the female parasite dies on site.
Following a period of 3 weeks, the larvae mature into adult mites, maintaining the infestation cycle.
The excretions of the mites and their decomposing bodies contain antigens which cause an immunological response (see type IV hypersensitivity reaction), presenting as severe pruritus and excoriations.
Clinical features
Intense pruritus, classically worse at night.
The name “scabies” comes from “scratch”
The warmth of the skin, especially under blankets and pajamas, can stimulate mite movement and activity, increasing pruritus.
Linear burrows (serpentine lines) found in intertriginous zones. t
Common sites: Interdigital web spaces, flexor surfaces of wrists, axillae, areolae, umbilicus, and genitalia.
Sparing of head and neck in adults (involved in infants and elderly).
Crusted (Norwegian) Scabies: Severe hyperkeratotic infection with thousands of mites; occurs in immunocompromised (HIV, elderly, Down syndrome). Minimal itching due to compromised immune response.