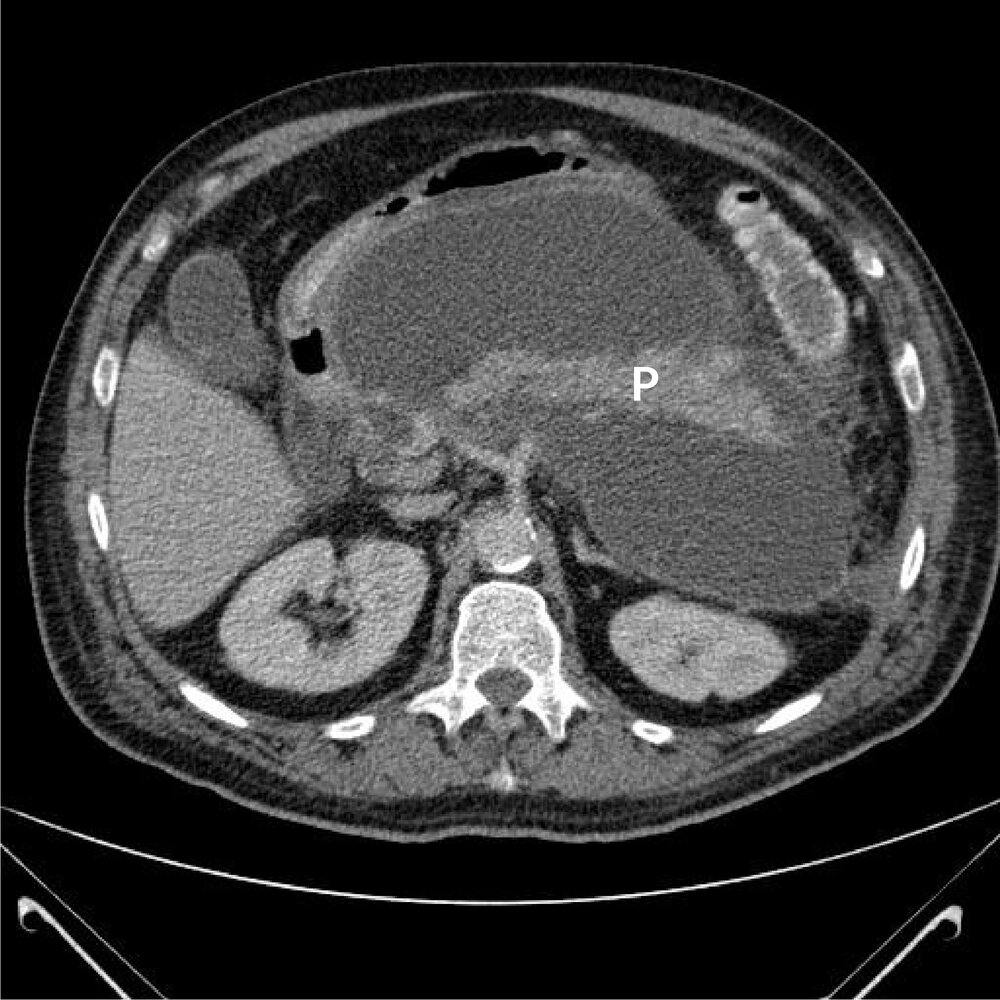
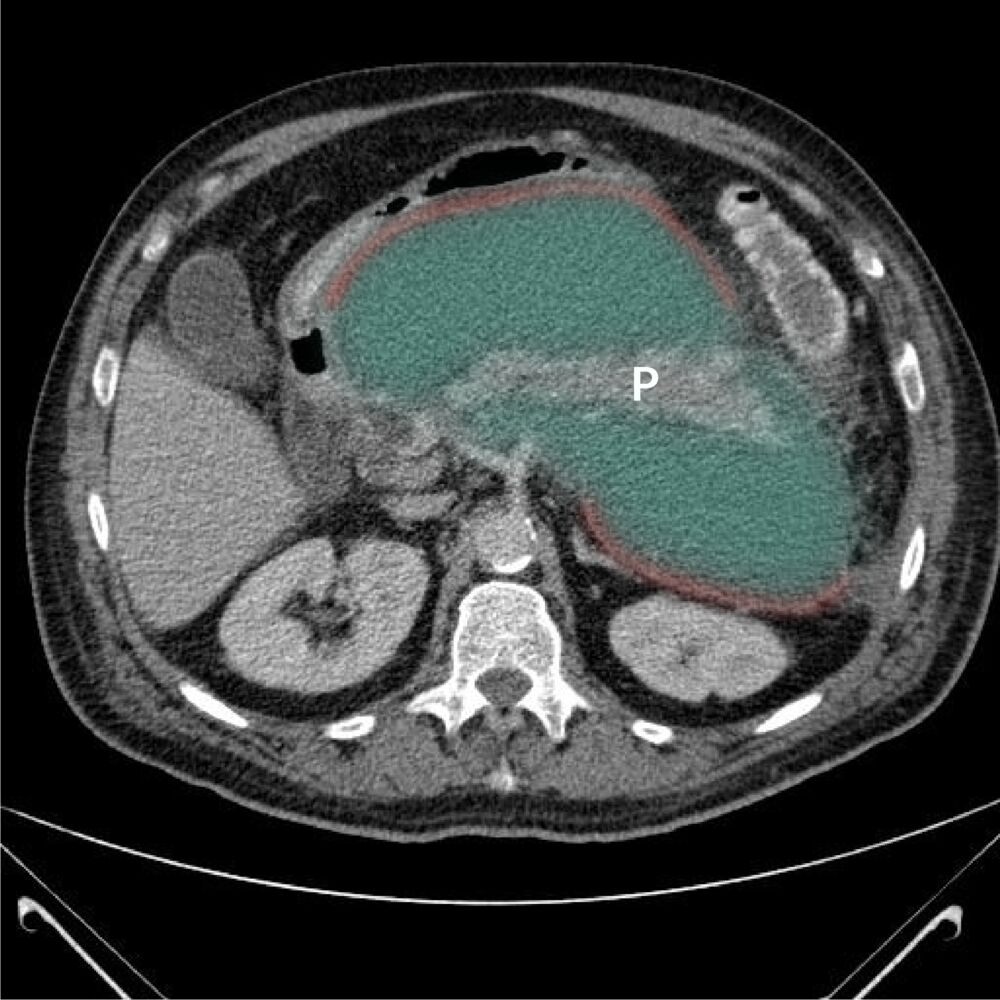
Symptomatic / > 6 cm / > 6 weeks: Drainage required (Percutaneous, Endoscopic Cystogastrostomy, or Surgical).
Diagnostics
Serum pancreatic enzyme levels: Lipase (specific) and amylase (nonspecific) are often normal.
Fecal elastase-1 (FE-1): most common test
Elastase is derived from a zymogen produced by pancreatic acinar cells and activated by trypsin in the duodenum; levels correlate with pancreatic exocrine activity. Therefore, low fecal elastase can help diagnose pancreatic insufficiency and supports a diagnosis of chronic pancreatitis.
Sudan staining (which identifies fecal fat)
Treatment
Exocrine Insufficiency (Malabsorption)
Pancreatic Enzyme Replacement Therapy (PERT) containing lipase, amylase, and protease.
Lipase is irreversibly inactivated at pH < 4.0. So use enteric-coated microspheres (delayed release) or PPI. t