Epidemiology
Etiology
Pathophysiology
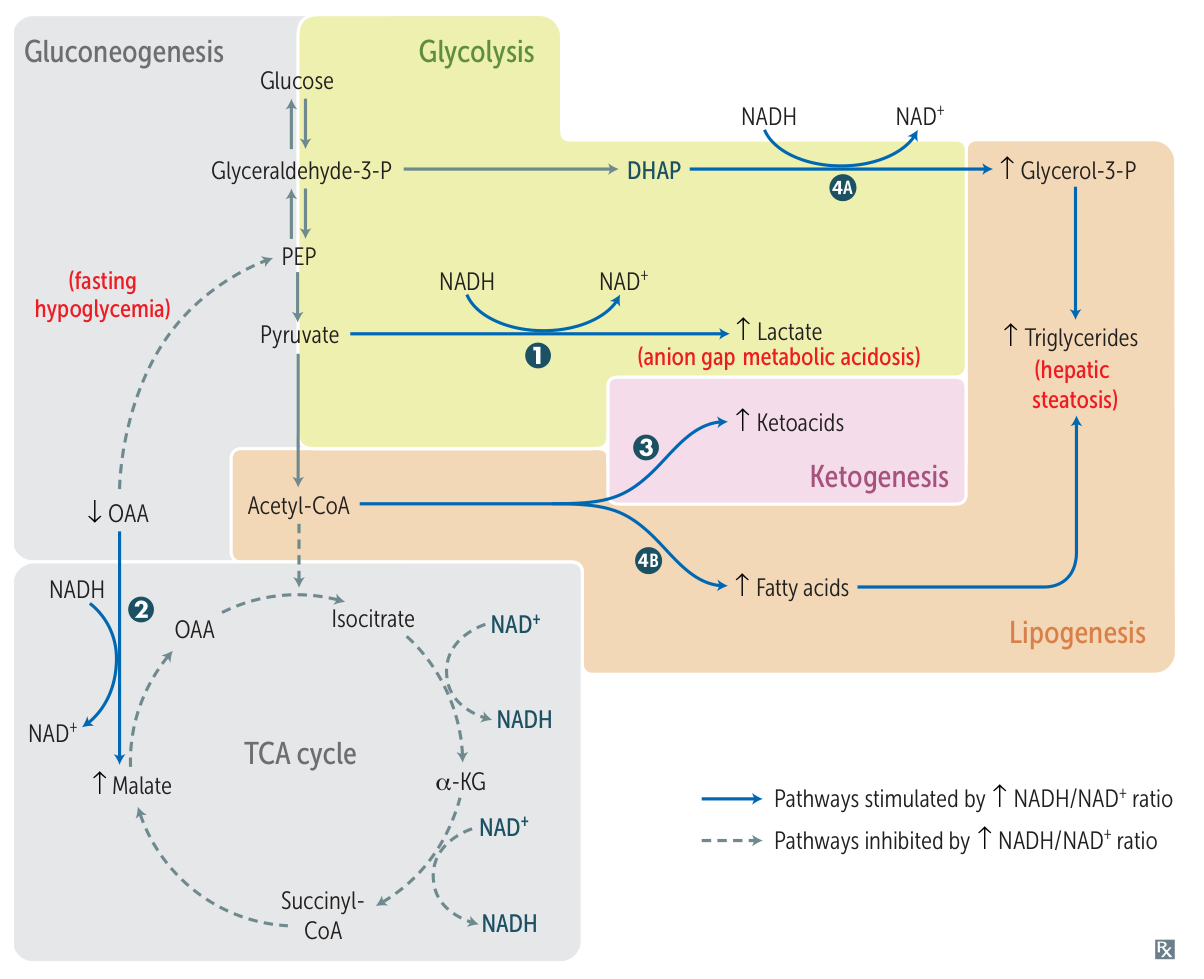
- Metabolic Imbalance: Metabolism by Alcohol Dehydrogenase (cytosol) and Acetaldehyde Dehydrogenase (mitochondria) ↑ NADH/NAD+ ratio.
- Consequences of ↑ NADH: ↓ gluconeogenesis (hypoglycemia), ↓ TCA cycle, ↑ fatty acid synthesis (lipogenesis) → Steatosis.
- Toxicity: Accumulation of Acetaldehyde causes direct hepatocyte damage and lipid peroxidation.
- Inflammation: CYP2E1 induction → ROS generation. Upregulation of TNF-α and IL-6.
- Fibrosis: Stellate cell activation (via cytokines/acetaldehyde) lays down collagen in Space of Disse.
Spectrum & Clinical Features
- Alcoholic Steatosis (Fatty Liver):
- Often asymptomatic.
- Reversible with cessation.
- Hepatomegaly.
- Alcoholic Hepatitis:
- Fever, RUQ pain, jaundice, tender hepatomegaly.
- May present with “bruit” over liver (rare).
- Alcoholic Cirrhosis:
Diagnostics
- Macrovesicular Steatosis: Hepatocytes filled with fat droplets displacing nucleus.
- Ballooning Degeneration: Hepatocyte swelling/necrosis.
- Mallory-Denk Bodies: Intracytoplasmic eosinophilic inclusions composed of damaged cytokeratin intermediate filaments.
- Neutrophilic Infiltrate: Characteristic of acute alcoholic hepatitis.
- Micronodular Cirrhosis: Small nodules (< 3mm) surrounded by fibrous bands (“hobnail” appearance).
Treatment